Continued from Part 1
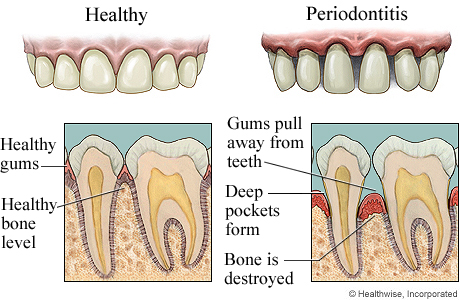
Diagnosis and treatment planning for bone defects and furcation involvement
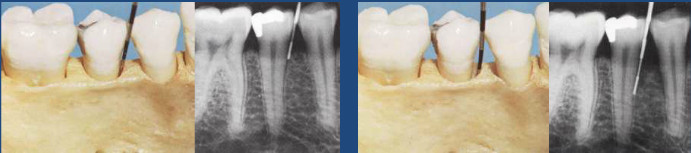 Careful radiographic or x-ray examination is done but it may not reveal the presence of a bone defect or its precise morphology.
Careful radiographic or x-ray examination is done but it may not reveal the presence of a bone defect or its precise morphology.
Direct examination of bone morphology:
- Lift a full thickness mucoperiosteal flap
- Granulations are curetted and root surfaces planed clean
- Alveolar crest examined, morphology of bone defect can be defined
- Mode of treatment decided Continue reading