
Class II molar relationship
Whether or not there is an increase in size or acceleration of growth of the mandible is one of the major controversies in functional appliance therapy. Although many researchers have claimed that the FR causes extra mandibular growth, this study showed that there were no significant differences between the FR and control groups as far as mandibular movement is concerned, the mean FR movement being 4.1 mm, standard deviation 3.0 mm; the control 5.0 mm, and standard deviation 2.6 mm. As the 5.0-mm change in the control was due to normal growth, it can be assumed that the 4.1-mm change in the FR group was no more than normal growth rather than any effect of the appliance. The maximum value seen in the control was 14.2 mm and for the FR it was 12.8 mm; again, because this change in the controls was due to normal growth it must be assumed that even the maximum FR change was no more than normal growth change. That the size of the mandible is unaffected with the FR is supported by evidence from Creekmore and Radney, and Hamilton et al., who found no significant differences between FR and untreated patient groups. Continue reading →
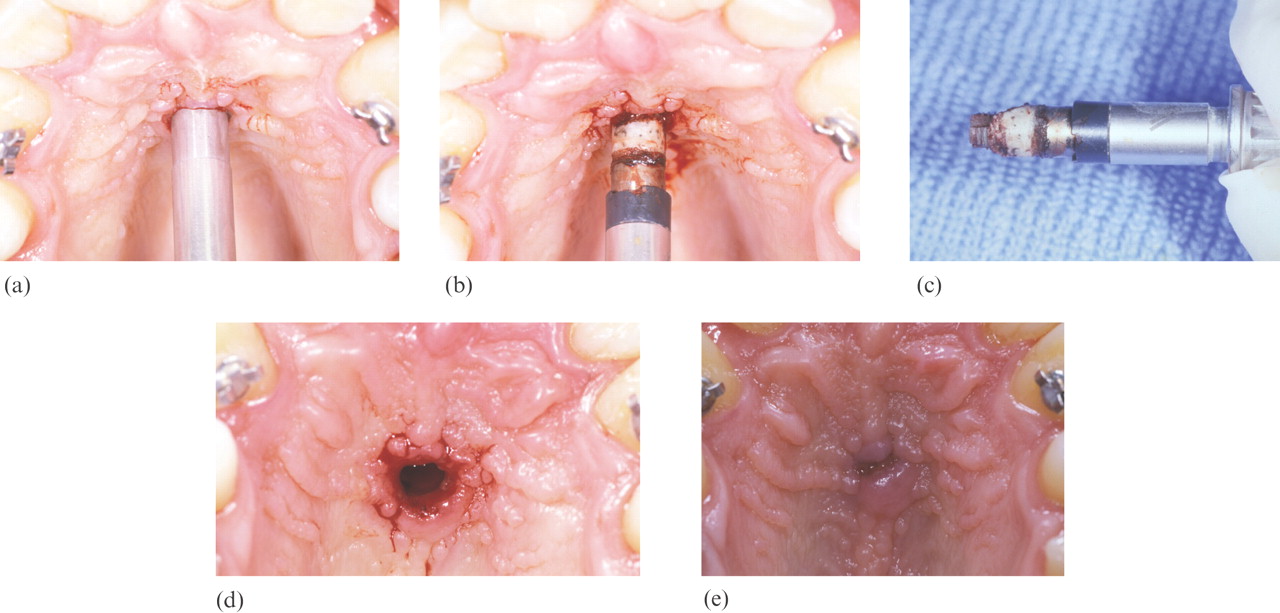 One of the limitations of using implants for orthodontic anchorage is having adequate bone. Conventional root-form implants require adequate thickness of bone for placement, thus limiting their use to edentulous areas. Several authors have reported the midsagittal area of the hard palate as a suitable site for a short implant. Continue reading
One of the limitations of using implants for orthodontic anchorage is having adequate bone. Conventional root-form implants require adequate thickness of bone for placement, thus limiting their use to edentulous areas. Several authors have reported the midsagittal area of the hard palate as a suitable site for a short implant. Continue reading 
