1.Attrition
2.Abrasion
3.Erosion
4.Abfraction lesions
5.Localized non-hereditary Enamel Hypoplasia
6.Localized non-hereditary Enamel Hypocalcification
7.Localized non-hereditary Dentin Hypoplasia
8.Localized non-hereditary Dentin Hypocalcification
9.Discolorations
10.Malformations
11.Amelogenesis imperfecta
12.Dentinogenesis imperfecta
13.Trauma
1. ATTRITION:
Defined as surface tooth structure loss resulting from direct frictional forces between contacting teeth.
Types of Attrition :
Proximal surface attrition
Occluding surface attrition
Treatment modalities:
Pulpally involved teeth should be Endodontically treated or extracted
Parafunctional activities i.e bruxism should be controlled
Myofunctional and TMJ problems should be resolved.
Occlusal equilibration
Rx –sensitivity
2. ABRASION:
The surface loss of tooth structure resulting from direct friction forces between the teeth and external objects or from frictional forces between contacting teeth components in the presence of abrasive medium.
Causes:
Tooth brush abrasion
Pipe smoking ‘depression abrasion’
Chewing tobacco
Forcing a tooth pick interdentally
Cutting, sewing thread with incisor teeth
Pica –syndrome.
TREATMENT:
Diagnose the cause and correct it
Prevent the patient from practicing the habits
Restorative therapy.
3.Erosion:
Loss of tooth structure resulting from chemico –mechanical acts in the absence of specific micro organisms.
Causes:
1 Ingested acids (citric acid)
2 Salivary citrates
3 Secreted acids (gingival crevice)
4 Mechanical abrasion
5 Microbial metabolic products – pyrophosphate
6 Acid fumes
7 Excessive tensile stresses at the tooth clinical cervix
8 Refused acids i.e regurgitation
Treatment:
Rx: Eliminate the cause and symptomatic Rx
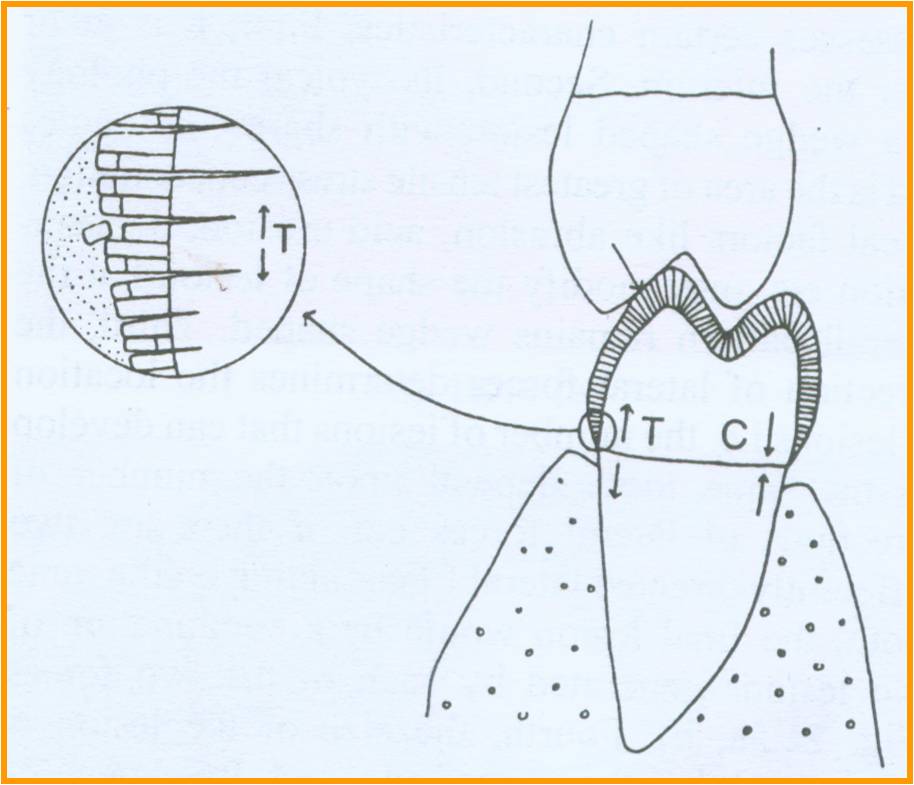
4. Abfraction lesions:
These are described as wedge shaped defects in the cervical region of the tooth and are hypothesized to be a result of tensile stresses concentrated in this area consequent to occlusal forces in some remote area
Mechanism for formation of abfraction lesions:
The ability of enamel to withstand stresses depends significantly on the direction of forces in respect to orientation of enamel rods. Forces are best withstood when they are in line with the rods, whereas under tensile forces that tend to pull the rods away from each other, enamel generally surrenders.
There occurs disruption of chemical bonds between hydroxyapatite crystals and as bonds are broken, small intercystalline spaces are created which allow penetration of water and other molecules. The disrupted crystalline structure is then much more susceptible to chemical dissolution and breakage from physical forces like brushing, compression, tension, mastication and bruxism
5.Localized Non – Hereditary Enamel Hypoplasia
The ameloblasts that are responsible for forming the enamel are very easily injured. During enamel formation. If these cells are irritated, their metabolic product i.e., the enamel matrix, will not be properly formed,
causing certain interruptions and defects. In certain areas, these defects will be apparent in the crown portion of the tooth (teeth) and this is called localized, non hereditary enamel hypoplasia.
Factors that can injure or destroy the ameloblasts during their formative activities. These include:
A Systemic disorders:
The most prominent of these are exanthemata disease, nutritional deficiencies (especially vitamins A, C, and D) and hypocalcemia from any cause, or a microbial process as in syphilis.
B. Localized disorders:
These include periapical infections of the preceding deciduous tooth (Turner’s hypoplasia), traumatic intrusion of the preceding deciduous tooth, etc.
C. Fluorides:
Treatment Modalities:
Selective odontotomy
Direct tooth – colored resinous materials
If the defect is in the occluding or contacting area, it is necessary to resort to metallic or cast restorations.
Lesions are discolored – Vital bleaching can be attempted
6. Localized Non-Hereditary Enamel Hypocalcification:
Just as destruction of the ameloblasts can interfere with the enamel matrix formation, it can also interfere with the mineralization of this matrix, this will lead to non-hereditary enamel hypocalcification.
Affected areas will not be defective in any way.
However, they will appear chalky and soft to indentation, and will be very stainable. Therefore, teeth shades change very fast from chalky to yellow, to brown, dark brown, and or grayish. If extensive, these lesions predispose to attrition and abrasion. Also, the enamel can be chipped if the lesion involves the entire surface of a tooth.
Treatment
Vital bleaching, laminated veneering, composite veneering, and porcelain fused to metal and cast ceramic crowns are the treatments to be pursued.
7. Localized Non-Hereditary Dentin Hypoplasia
The ameloblasts are irreplaceable cells, and their disappearance means no enamel in this particular area. However, the odontoblasts are replaceable cells. If they disappear. There will be no dentin temporarily, but dentin deposition will be resumed as soon as other pulp cells start depositing it. In these cases, the defect will be isolated within the dentin substance
There will be no apparent destruction to be diagnosed or treated.
8. Localized Non-Hereditary Dentin Hypocalcification
These defects have same causes as hypoplasia. Even though the dentin will be present in substance it will be softer, more penetrable, and less resilient.
9. Discolorations
10. Malformation
Malformation should be differentiated from the illusion that can occur when there is a substantial discrepancy between tooth size and jaw size.
 11. Amelogenesis Imperfecta:
The abnormality could be in the matrix formation leading to hypoplasia or it could be in the mineralization leading to hypomineralization.
These lesions usually affect one type of dentition, and only the enamel
Treatment Modalities:
Selective odontotomy
Full veneering includes procedures with metallic, metallic based, or cast ceramic restorations.
12: Dentinogenesis Imperfecta Or Hereditary opalescent dentin.
The color may be from grey, brown, yellow-brown to violet.
Most of them exhibit a translucent hue.
The enamel, although intact, is easily chipped because of the defective dentino –enamel junction.
The crowns are overcountered.
The roots are short and slender
There are signs and symptoms of extensive attrition.
The dentin is devoid of tubules.
The dentin contains a lot of inter globular dentin.
The decay process, if initiated, will spread laterally.
Root canal and pulp chamber space is obliterated
Dentin hardens and resilience is almost half that of normal dentin.