
© mund-kiefer-gesicht-bremen.de
The prosthetic replacement of lost teeth frequently, though not necessarily, involves surgical preparation of the remaining soft tissues in the mouth. The aim is to leave a satisfactory base for subsequent placement of prosthetic appliances to enable an edentulous or toothless individual to live comfortably with functioning dentures.
Ideally treatment for these procedures should be planned jointly (by a prosthodontist and oral surgeon). However many procedures of preprosthetic surgery are becoming history due to advancements made in dental science such as the introduction of dental implants.
Preservation of alveolar ridge (gum ridge) at time of extraction of teeth
© maxillofacial.com
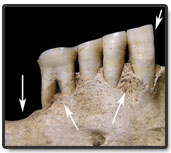
Preservation of alveolar ridge or the ridge that forms the borders of the upper and lower jaws and contains the sockets of the teeth for prosthesis start when the first permanent tooth is extracted itself. Careful planning has to be done during removal of buried teeth and lesions. Difficult extractions (multi-rooted teeth) are best removed by transalveolar extraction (extraction that involves removal of bone surrounding the tooth) to avoid alveolar or jaw fracture. The common site of fracture is the buccal or bone plate facing the cheeks opposite the upper molars.
Access to deeply buried roots is made through lateral aspect of the alveolus leaving the ridge intact. Bone cutting should be limited to one side. A more conservative approach is important where periodontal disease has already caused more bone loss in the mouth. It should be remembered that alveolar bone once lost cannot be replaced.
Preservation of alveolar bone in edentulous or toothless patients
The natural process of bone resorption in the mouth makes the alveolar ridge weaker. Symptomless root fragments and buried teeth unlikely to come to surface during their lifetime need not be extracted. On the other hand, teeth lying superficially and those associated with cysts and granulomas can be extracted.
Preprosthetic surgical techniques
Surgery involving bone irregularities
- Alveoloplasty
- Tori removal
- Maxillary tuberosity reduction
- Mylohyoid ridge reduction
- Genial tubercle reduction
Surgery involving soft tissues irregularities
- Maxillary tuberosity reduction (soft tissue)
- Frenectomy
- Denture irritation hyperplasia
- Flabby ridge
- Papillary hyperplasia
Alveoloplasty
© toothiq.com
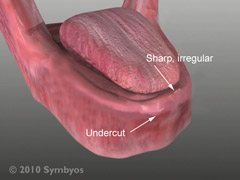
Alveoloplasty is a minor surgical procedure done to smoothen irregular ridges and remove undercuts from the gum ridge.
- Local anesthesia is administrated. A horizontal incision is made on the alveolus, with vertical releasing incision if needed, under local anesthesia.
- Gum flap is reflected to expose the alveolar crest.
- The excess bone is trimmed with a large rosehead bur or a bone ronguer and then smoothen with a bone file.
- The operator then replaces the gum flap and runs his or her finger over the gum ridge to check for smoothness.
- The procedure is followed by irrigation with saline and suturing.
Tori removal
© exodontia.info
Tori are bony exostoses (benign outgrowth from a bone) found in both jaws. Palatal tori are found in the centre of the hard palate and the lingual tori on the lingual premolar or molar region of the lower jaw. Both tori are normal anatomical variants in the mouth. Palatal tori should be removed if they cause denture instability, or repeated fracture or where there is soft tissue trauma.
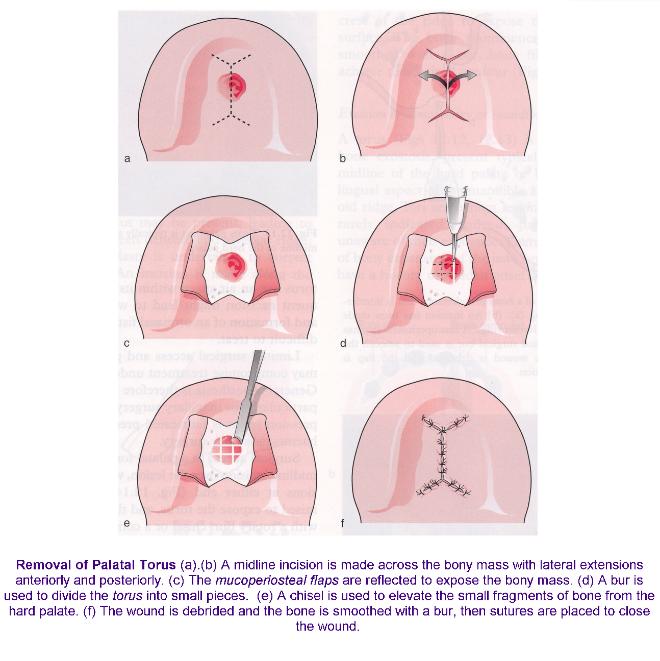
Removal of palatal tori
- Local anesthesia is administrated. Reflection of mucoperiosteal flaps is done with Y-shaped incisions on the palate.
- Sectioning of torus is done with a fissure bur.
- A small osteotome is used to remove sections of the torus.
- A large bone bur is used to produce the final desired contour.
- Excess soft tissue is removed and flap closure is done.
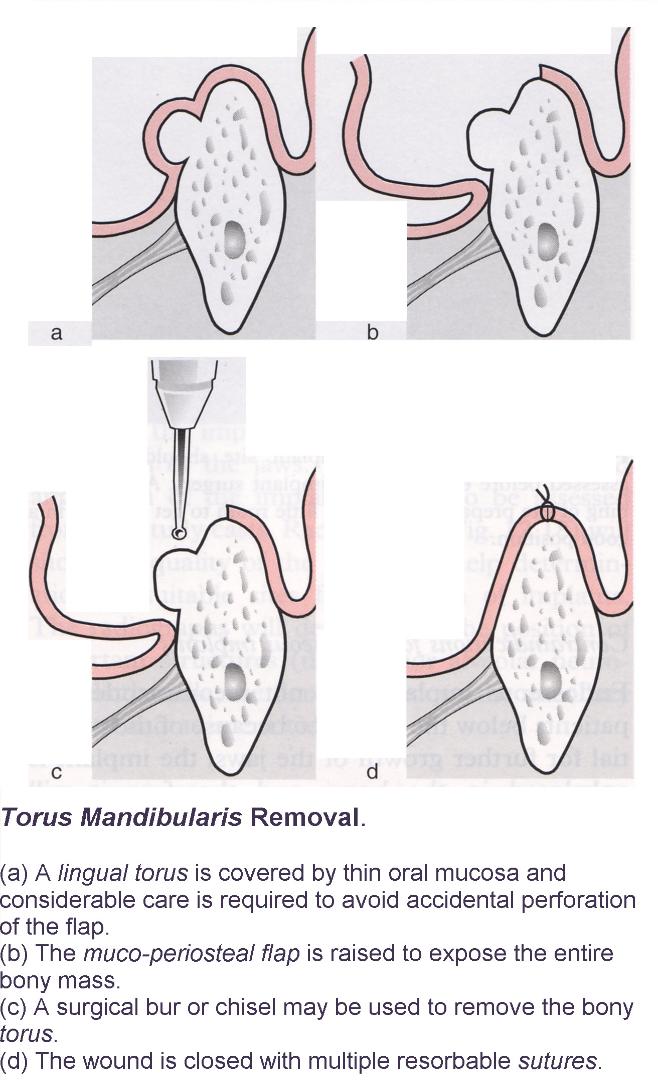
Removal of lingual tori
© exodontia.info
- Local anesthesia is administrated. An incision is made on the torus.
- The torus is exposed.
- A trough is created between the lower jaw and torus using a fissure bur.
- Removal of torus is done with an osteotome.
- A bone bur is used to get the final desired contour.
- Soft tissue closure is done.
Maxillary tuberosity reduction
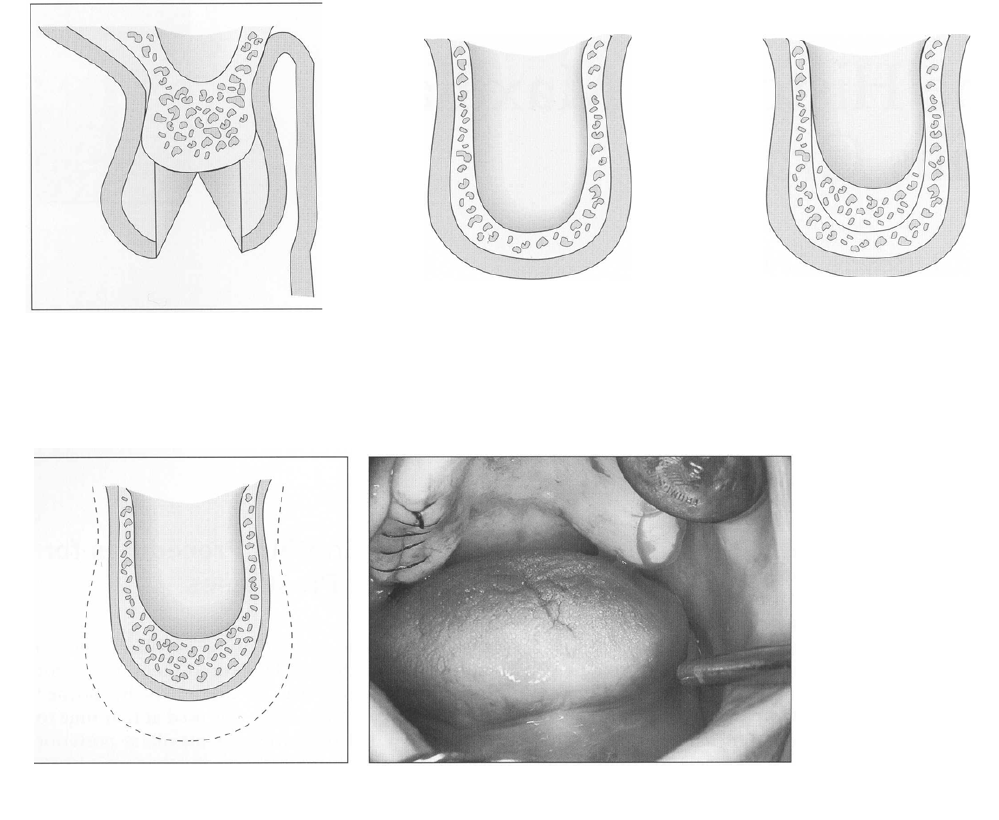 The maxillary tuberosity is the bony protuberance at the end of the upper jaw. Reduction of the maxillary tuberosity is done to improve retention of the upper denture.
The maxillary tuberosity is the bony protuberance at the end of the upper jaw. Reduction of the maxillary tuberosity is done to improve retention of the upper denture.
- Local anesthesia is administrated. Incision is made extending along the crest of alveolar ridge distally to the superior extent of tuberosity area.
- Elevation of mucoperiosteal flap is done.
- Elimination of bony excess is done using bone rongeur and after the desired contour is obtained, suturing is done.
- A cross sectional view of the posterior tuberosity area will show a vertical reduction of bone and reapposition of gum flap.
- If the maxillary tuberosity is perforated and the sinus floor is not violated, no specific treatment required. Initial denture impression can be made 4 weeks after surgery. In case of sinus infections, antibiotics and sinus decongestants should be given 7 to 10 days post operatively. Patient has to be cautioned against creating excessive sinus pressure, such as nose blowing or sucking with a straw for 10 to 14 days.
To be Continued in Part 2.