The inferior alveolar nerve (sometimes called the inferior dental nerve) is a branch of the mandibular nerve, which is itself the third branch (V3) of the trigeminal nerve (cranial nerve V).
Path
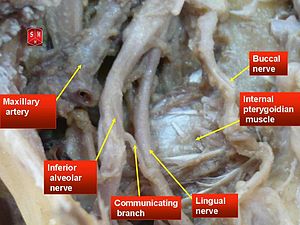
Relative position of inferior alveolar nerve
Before traversing the mandibular foramen, it first gives off the nerve to the mylohyoid, a motor nerve supplying the mylohyoid and
the anterior belly of the digastric. It then enters the mandible via the mandibular foramen.
While in the mandibular canal within the mandible, it supplies the mandibular (lower) teeth with sensory branches that form into the inferior dental plexus and give off small gingival and dental nerves to the teeth.
Anteriorly, the nerve gives off the mental nerve at about the level of the mandibular 2nd premolars, which exits the mandible via the mental foramen (supplying sensory branches to the chin and lower lip).
The inferior alveolar nerve continues anteriorly as the mandibular incisive nerve to innervate the mandibular canines and incisors.
Anatomical variations
Different variations in the course of the inferior alveolar neurovascular bundle are described (Anderson & Kosinski 1991). The classification by Carter and Keen (1971) in the mandible is illustrated in picture attached to this article . These results were obtained from only eight dissected mandibles. In another larger study the course of the IAN was evaluated from 3612 radiographs (Nortje et al. 1977). The radiographs were divided into four categories:
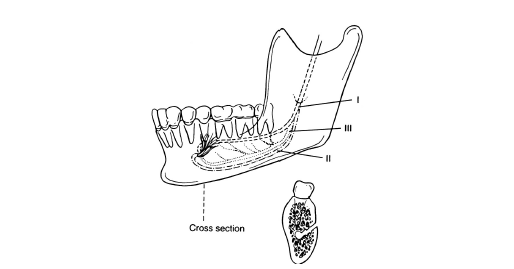
Classification of inferior alveolar nerve positions
1) high mandibular canals (within 2mm of the apices of the first and second molars),
2) intermediate mandibular canals,
3) low mandibular canals, and
4) other variations – these included duplication or division of the canal, apparent partial or complete absence of the canal or lack of symmetry.
Of the 3612 subjects, 47% of the canals were high, 49% were low, and only 3% could not be fitted into the high or low canal categories. The main conclusion of this study was, that the mandibular canals are usually, but not invariably, bilaterally symmetrical, and the majority of hemimandibles contain only one major canal.
Multiple mandibular canals of the bifid variety characterized by a single mandibular foramen and two nearly equal canals are unusual. In the study of Nortje and co-workers, duplication or division of the canal was found in 0,9% (33/3612) of the cases
in the panoramic radiographs in otherwise normal patients (Nortje et al. 1977). In another study only 0.08% bifurcation of the IAN in 5000 US Army recruits, aged 17 to 26, was found (Grover & Lorton 1983). Furthermore, Langlais and co-workers (1985)
evaluated routine panoramic radiographs of 6000 patients, and they found 57 (0.95%) cases of bifid inferior mandibular canals, 19 in males and 38 in females. However, no cases of multiple canals in orthognathic surgical cases have been reported.
Anesthesia

Local anesthesia must be applied to the ramus region to be effective
Administration of anesthesia near the mandibular foramen causes blockage of the inferior alveolar nerve and the nearby lingual nerve (supplying the tongue). This is why the numbing of the lower jaw during dental procedures causes patients to lose sensation in:
- their teeth (inferior alveolar nerve block)
- their lower lip and chin (mental nerve block)
- and The Anterior Two-Thirds Of the Tongue Of the same Side (lingual nerve block).
Inferior alveolar nerve injury
Now that we have discussed the anatomy of the inferior alveolar nerve, we will turn to the dental procedures that cause inferior alveolar nerve injury:
- 1) Negligent Implant Placement
- 2) Negligent Root Canal Treatment
- 3) Negligent Fracture Of The Mandible
- 4) Local Anesthetic
- 5) Negligent Surgical Extraction of Lower Molars
1) Negligent Implant Placement
The most common dental procedure which causes injury to the inferior alveolar nerve is the placement of a posterior implant in the mandible (back of the lower jaw). The dentist can injure the inferior alveolar nerve in a number of ways during an implant procedure, but it all boils down to one fact, he/she doesn’t know where the inferior alveolar nerve is. When a patient presents to the dentist and wants an implant to support an implant crown to replace a missing second molar in the posterior mandible, the dentist needs to determine the size and the width of the implant thay are going to place in this edentulous (open/missing tooth) space. The dentist knows that the inferior alveolar nerve is somewhere below where the missing second molar use to be and that every effort must be made to avoid injuring that nerve when placing the longest implant possible to ensure the future success of the implant. The dentist has been taught that he/she should provide a safety clearance of 2mm above the mandibular canal, so that the drill or implant does not injure the inferior alveolar nerve, and also to keep well clear of the mental nerve foramen.
In order to determine the relationship of the inferior alveolar nerve to the alveolar crest (top of the bone in the space of the missing second molar) or to determine the relationship of the third molar to the inferior alveolar nerve, panorex x-rays or a periapical x-rays are used as screening readiographs to gage the appropriate length of an implant or the risk of injury to the inferior alveolar nerve during a third molar extraction. Both of these radiographs are two dimensional images and may provide incomplete radiographic information and may distort the anatomy with regards to the location of the inferior alveolar
nerve. If these screening radiographs provide incomplete information determine where the alveolar nerve is in relation to the alveolar crest or demonstrate a close relationship of the third molar to the inferior alveolar nerve, the dentist must not guess where the inferior alveolar canal is and should refer the patient for a Cone Beam CT scan.