Continued from Part 1
Components of implants

© http://www.orofacialsurgery.com.sg
Implant
Implant is the endosteal (within bone) material that is placed within the bone during stage 1 dental implant surgery. It is either titanium or titanium alloy, with or without hydroxyapatite coating.
Cover screw
A screw is placed in the implant during the healing phase after stage 1 surgery. This crew is usually to facilitate easy suturing of the soft tissue over the implant. At stage 2 dental implant procedure screw is removed and replaced with subsequent components.
Healing cap
Healing cap is a dome-shaped screw that is placed after stage 2 surgery and before prosthesis placement. The cap may be made out of resin, such as polyoxyethylene, or one of the titanium metals.
Abutment
Abutment is that component of the implant system that screws directly into the implant. The abutment will eventually directly support the prosthesis. It is smooth, polished straight-sided titanium. The length may range from 1 to 10 millimeters.
Impression post
The impression post facilitates the transfer of intra oral location of fixture or abutment to a similar position in the laboratory cast. Impression post is then removed from the mouth and joined to the lab analogue before being transferred into the impression.
Laboratory analog
Laboratory analog is a component machined to exactly represent either the implant or the abutment in lab cast.
Waxing sleeve
Waxing sleeve is attached to the abutment by the prosthesis=retaining screw on a lab model. Waxing sleeve will eventually become a part of the prosthesis. It may be a plastic pattern that is burned out inside the investment and replaced by a cast precious alloy.
Prosthesis-retained screw
Prosthesis-retaining screw penetrates the fixed restoration and secures it to the abutment. In non-segmented restorations the screw tightens the abutment directly to implant. The screw can be made of titanium, titanium alloy, or gold alloy.
Implant material
Titanium
Titanium is the best material available at present. It oxidizes in the atmosphere to form an inert surface layer of titanium oxide. It has good mechanical properties. Other materials – niobium, hydroxyapatite are well-tolerated.  Hydroxyapatite can be used as coating which is osteoinductive. Aluminum oxides, cobalt-chrome, molybdenum ad stainless steels are less tolerated.
Examination of implant site
Clinical examination
Visual inspection and palpation is done to check for flabby excess tissue, narrow bony ridges, sharp underlying ridges and undercuts.
Radiographic examination
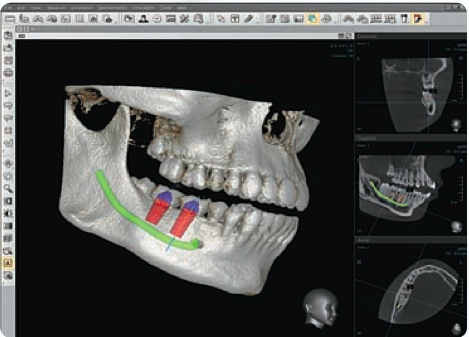
CT scan © http://www.orofacialsurgery.com.sg
- Orthopantomograph (OPG) – to assess vertical bone height,
- Lateral cephalometric film – width of front upper jaw and lower jaw,
- CT scan – to locate inferior alveolar canal and upper jaw sinus and to evaluate ridge form
Study casts
Duplicates can be used for diagnostic wax-up so that the tooth position can be planned. A template can be made with indicator holes drilled as an aid to the surgeon so that the implants are placed in optimal position.
Principles of dental implant surgery
First surgical phase (implant placement)

© http://www.orofacialsurgery.com.sg
Under local anesthesia the dentist places dental implants into the jaw bone with a very precise surgical procedure. The implant remains covered by gum tissue while fusing to the jaw bone.
Second surgical phase (implant uncover)
The length of time necessary to achieve integration varies from site to site. After satisfactory integration of implant uncovering of implant is done to attach the abutment to it with preservation of attached tissues.
Prosthetic phase
Once the gums have healed, an implant crown is fabricated and screwed down to the implant.
Post operative care
Implant survival depends on proper and timely home care and maintenance. The goal of implant maintenance is to eradicate microbial population. Recall visits should be scheduled at least every 3 months for the first year. The area surrounding the implant should be removed of calculus by using plastic or wooden scalers. A rubber cup with low abrasive polishing paste or tin oxide may be used to polish implant abutments.
Points to be evaluated during recall:
- Mobility of implant,
- bleeding,
- framework fit,
- occlusion
Problems involved in dental implants placement
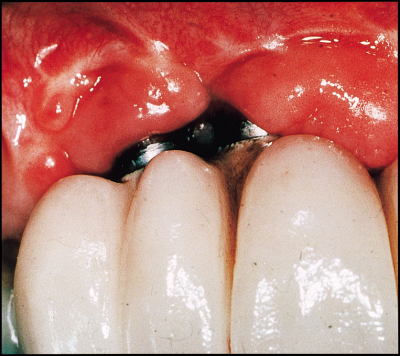
Poor positioning of implants © nature.com
- Improper angulation of implant
- Improper position of implant
- Perforation of maxillary sinus
- Perforation of inferior alveolar canal
- Dehiscence (splitting up) of bucco-cortical or linguo-cortical bone plate
- Lower jaw fracture (in case of thin lower jaw)
- Soft tissue wound dehiscence
Criteria for success of implants
- The individual unattached implant is immobile when tested clinically
- No evidence of peri-implant radiolucency is present as assessed on an undistorted radiograph
- The mean vertical bone loss should be less than 0.02mm annually after the first year of service
- No persistent pain, discomfort or infection is attributable to implants
- The implant design does not preclude placement of a crown or prosthesis with an appearance that is satisfactory to the individual and the dentist.
Nice description. It provides lot of information. Can you suggest me these surgeries are safe or some side effect in feature? How much time it taken.
Thanks.