DEFINITION
According to the Glossary of Prosthodontic terms – 7
Full veneer crown is described as “A restoration that covers all the coronal tooth surfaces (Mesial, Distal, Facial, Lingual and Occlusal)â€
REVIEW OF LITERATURE
H .T. Shillingberg, S . Hobo ,D . Fisher (1973) conducted a study on “ Preparation design and margin distortion in porcelain fused to metal restorationâ€
They concluded that the shoulder finish lines with or without a bevel were found to produce significantly less distortion in labial margins in porcelain fused to metal restoration than do chamfer finish lines with or without a bevel.
J.R.Gavelis ,J.D.Morency ,E.D.Riley ,R.B.Sozio (1981) conducted a study on “The effect of various finish line preparation on the marginal seal and occlusal seat of full crown preparationsâ€
They concluded that the feather edge and parallel bevel preparation demonstrated the best marginal seal, followed in order by the full shoulder ,45 degree shoulder and 90 degree shoulder with 30 and 45 degree bevel.
D.L.Koth (1982) conducted a study on “ Full crown restorations and gingival inflammation in a controlled populationâ€
A Periotron instrument was used to quantitate the volume of crevicular fluid present in the gingival sulcus.38 full crown restorations were compared to non restored teeth in the same patient. He concluded that
The full crown restoration have the potential for causing gingival inflammation. However they need not be associated with a significant increase in gingival inflammation.
Gingival inflammation surrounding full crown restoration may be controlled regardless of gingival margin placement, when the gingiva is healthy and restorations are adequate.
P. J. B. Leempoel, L. M. Leemens, P. A. Snoek, M.A.Vant Hoff (1987) conducted a study on “The convergence angle of tooth preparation for complete crowns†and concluded that overall convergence angle of 15.5 to 30.2degrees provide sufficient retention for an artificial crown.
W.A.Kent , H.T.Shillinberg ,M.G.Duncanson (1988)conducted a study on “taper of clinical preparation for cast restoration†and concluded that means of taper preparation done by an experienced operator ranged from 8.6 to 26.6 degrees. The overall mean was 14.3 degree.
Internal features such as grooves and boxes have a significant lower degree of taper 7.3 degrees as compared to external axial walls.
C.J.Goodacre , W.V.Campagni , Steven A. Aquilino (2001) conducted a study on “ Tooth preparation for complete crowns: an art form based on scientific principles†and concluded that
-the total occlusal convergence angle should range between 10-20 degrees.
-the minimum occlusocervical dimention for molars should be 4 mm when prepared with 10-20 degrees taper.
-the ratio of occlusocervical to faciolingual dimention should be at least .4 or higher for all teeth.
-whenever possible while preparing tooth the facio and linguoproximal corners should be preserved therby enhancing resistance form.
-When tooth conditions and aesthetics permit, finish lines should be located supragingivally.
-teeth lacking adequate resistance form should be modified with the creation of grooves/boxes.
-axial grooves/boxes should be routinely prepared for mandibular molars and should be located in proximal surface.
-chamfer finish lines approximately .3mm deep are well suited for all metal crowns.
-both shoulder and chamfer finish lines can be used with all ceramic crowns if they are bonded to the prepared tooth.
-smooth tooth preparation appears to enhance the fit of restoration.
-line angles should be rounded on all ceramic tooth preparation to reduce stress in the restoration.
COMPLETE CAST CROWN
INDICATIONS
On teeth that exhibit extensive coronal destruction
On Non-esthetic zone teeth with extensive restorations
Short clinical crowns
Retainer for a long span fixed partial denture
On endodontically treated teeth
To Support removable partial denture where necessary contours with a partial coverage restoration is difficult.
In cases of generalized attrition where vertical dimension is reduced.
CONTRAINDICATIONS
If treatment objectives can be met with a more conservative restoration
Extensively restored or cariously involved teeth within esthetic zone
ADVANTAGES
Greater retention and resistance than a more conservative restoration
Strength is superior to that of other restoration
Permits easy modification of the occlusion
Protects the coronal integrity of a natural tooth compromised by restorations
DISADVANTAGES
Removal of tooth structure is extensive and can have adverse effects on the periodontium
It is no longer feasible to perform electric vitality testing of the abutment tooth
TOOTH PREPARATION
ARMAMENTARIUM
Handpiece
Round ended tapered diamond
171L bur
Torpedo diamond
Torpedo bur
Short needle diamond
Red utility wax
Procedure of tooth preparation
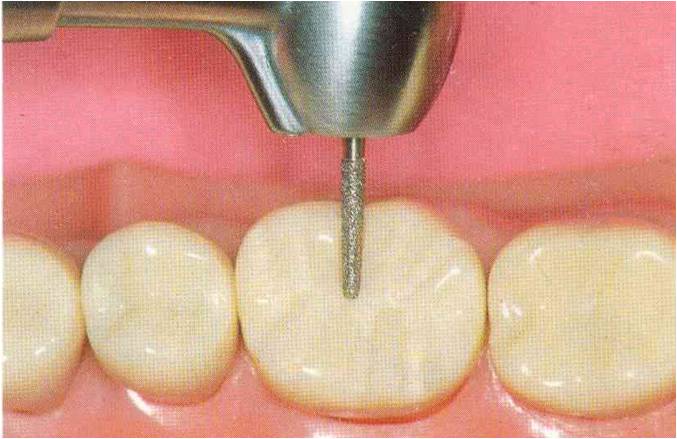
Place the round ended tapered diamond bur approx . 1mm deep in central , mesial , and distal fossae, and creating about 1.5 mm of clearance on the functional cusps and 1mm on the non-functional cusps.

Place these grooves in the buccal and lingual developmental grooves and in each triangular ridge extending from the cusp tip to the centre of its base.
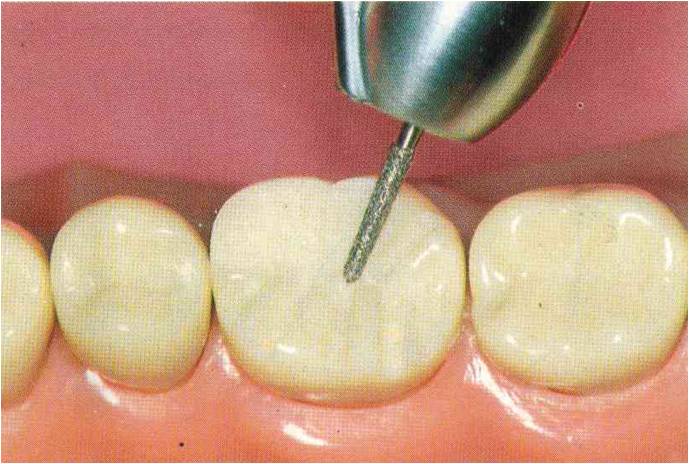
On the non-functional cusp, the groove should parallel the intended cuspal inclination, on the functional it should be slightly flatter to ensure additional reduction of the functional cusp.
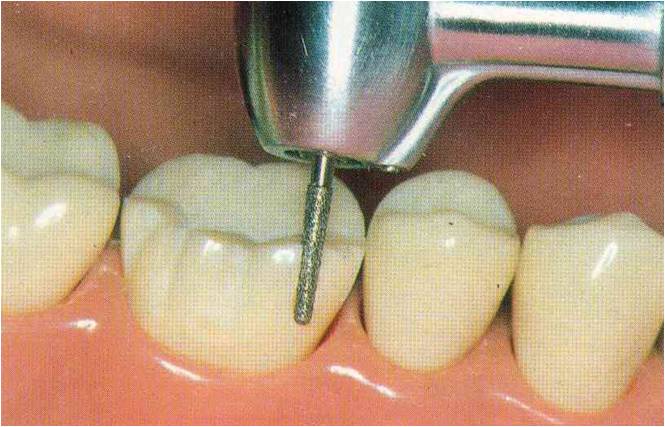
Place depth orientation grooves for a functional cusp bevel across the facial occlusal line angle of the mandibular premolar or molar, and across the lingual occlusal of a maxillary tooth
Round ended tapered diamond is used to give bevel parallel to the inward facing inclines of the opposing tooth, at a depth of 1.5mm, usually forming a 45 degree angle with the axial wall.
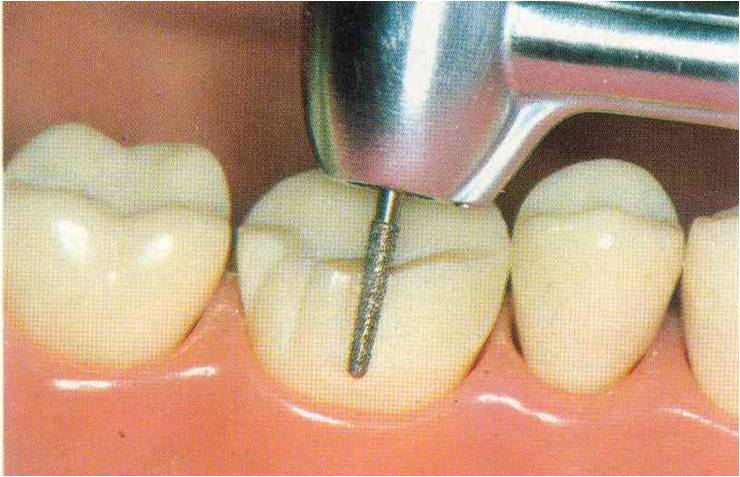
Complete the occlusal reduction in two steps. Half of the occlusal surface is reduced first so that the other half will be maintained as reference.
After completing the occlusal reduction the clearance can be checked by having the patient to close on a 2mm thick strip of red utility wax.