Continued from Part 2
© chiro.org
Temporomandibuar joint
Pain from the temporomandibular joint may result from dysfunction, trauma, acute or chronic inflammation, or primary or secondary cancerous tumors. Examination may reveal the masticatory (chewing) muscles tender to palpation or occasionally the joint swollen and warm to touch or tender to palpation via the external auditory meatus. Pain from the temporomandibular joint:
-
Is usually dull
-
Is usually caused by muscle spasm
-
Is usually poorly localized
-
May radiate widely
-
Is usually intensified by movement of the lower jaw
-
May be associated with trismus (limited mouth opening) because of the spasm in the masticatory muscles
Salivary glands
Examination usually reveals the salivary gland swollen and sensitive to palpation. In acute parotitis (inflammation of the parotid gland), mouth opening causes severe pain, and thus there is a degree of limited mouth movement. Salivary flow from the affected gland is usually reduced. Pain may be associated with fever and body discomfort. In children, the most common cause is mumps. In adults, the pain from salivary glands results usually from blockage of a salivary duct by calculus or a mucous plug or sialadenitis (gland inflammation), when pus may ooze from the duct opening.
Pain from salivary glands:
-
Is localized to the affected gland
-
May be quite severe
-
May be intensified by increased salivation, such as before and with meals – the pain may wane in the minutes or hours following salivary stimulation.
Sinuses and pharynx

© sinus-symptoms.net
Disease of the paranasal sinuses and nasopharynx can cause oral and/or facial pain. In acute sinusitis there has usually been a preceding ‘cold’ followed by local sinus pain and tenderness (but not swelling) and radio-opacity of the affected sinus, sometimes with an obvious fluid level. Transillumination from a light in the oral cavity may show a fluid level.
With maxillary sinusitis, pain may be felt in related upper molars and premolars, any of which may be tender to percussion. The pain of ethmoidal or sphenoidal sinusitis is deep in the nose. Pain in any type of acute sinusitis may be aggravated by a change of position of the head.
Tumors of the sinuses or nasopharynx can also cause pain on face. These tumors are often carcinomas that infiltrate various branches of the trigieminal nerve and can remain undetected until too late. Nasopharyngeal carcinoma often presents late, with facial pain, paraesthesia (partial numbness), deafness on one side and/or of cervical lymph node enlargement (Trotter syndrome).
Pressure on the mental nerve
Rarely, pain is caused by pressure from a denture on the nerve, which comes to lie on the crest of the ridge as the alveolar bone is resorbed in the toothless lower jaw. Either the denture should be relieved from the area or occasionally, it is necessary to re-site the nerve surgically.
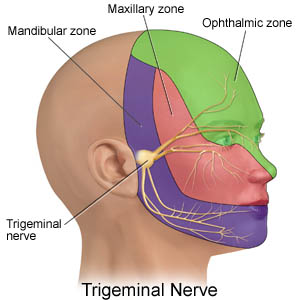
Neurological (neuropathic) causes of orofacial pain
© drugs.com
Sensory innervations of the mouth, face and scalp depends on the trigeminal nerve, so that disease affecting this nerve can cause orofacial pain or indeed sensory loss – sometimes with serious implications.
Facial neuralgia caused by tumors or other lesions
Any lesion affecting the trigeminal nerve, whether it be traumatic, cerebrovascular disease, multiple sclerosis, infections such as HIV / AIDS, inflammatory or neoplasmatic (for example a nasopharyngeal or antral cancer), may cause pain, often with physical signs, such as facial sensory or motor impairment.
Idiopathic trigeminal neuralgia
Severe piercing orofacial pain on one side of the face may be of unknown origin, and in the absence of identifiable organic cause is termed ‘idiopathic trigeminal neuralgia’. Similar pain is experienced in the rare idiopathic short-lasting, one-sided, neuralgiform headache attacks with tearing of the eyes.
Other neuralgias
Glossopharyngeal and post-herpetic neuralgias may also cause pain.
Vascular cause of orofacial pain
Several disorders in which the most obvious organic feature is expansion or constriction of the blood vessels can cause orofacial pain. The pain is usually obviously in the face or head rather than In the mouth, but occasionally can involve both, and can be difficult to differentiate from other causes of orofacial pain. These include:
-
Migraine, migranious neuralgia, giant cell arteritis
A rare condition term neuralgia-inducing cavitations osteonecrosis, related to disorders in blood coagulation, may also cause jaw pain.
Other organic causes of headache or orofacial pain

© Royalty-Free/Corbis
Headache or orofacial pain is occasional the presenting feature of:
-
Exertion (including postcoital headache)
-
Fevers
-
Hypertension
-
Meningeal irritation: severe headache with nausea, vomiting , neck pain or stiffness (with inability to kiss the knees) or pain on raising the straighten legs (Kernig sign) implies meningeal irritation. Urgent neurological attention is needed, since the pain indicate meningitis, metastases or subarachnoid hemorrhage.
-
Raised intracranial pressure: this is one is the most serious, but also the least common causes of headache. The headache is severe, worse on waking and decreased during the day. It is aggravated by straining, coughing, sneezing or lying down. Nausea and vomiting are common. Neurological attention and examination for papiloedema is essential, since this may be caused by malignant hypertension, a tumor, abscess or hematoma. When no specific cause can be found it is termed ‘idiopathic (benign) intracranial hypertension’ which may be precipitated by tetracyclines, vitamin A, nitrofurantoin and nalidixic acid and is associated with partial thrombosis of the superior sagittal sinus.
-
Chronic obstructive airways disease
-
Some endocrinopathies, such as diabetes
-
HIV infection
-
Drug use (for example phenothiazines)
-
Paget’s disease
To be continued in Part 4