Continued from Part 3
What are the investigations needed for oral cancer?

© flickriver.com
Investigations are done to see the extent of cancer and to confirm the diagnosis. The following investigations may be indicated:
- Jaw radiography or x-ray
- Chest x-ray or computed tomography (CT). This is important as a pre-anesthetic check especially in individuals with known airways disease, and to demonstrate second primary tumors or spread to lungs or lymph nodes, ribs or vertebrae.
- Magnetic resonance imaging (MRI) or CT of the primary site, of the head and neck, and suspected sites of distant spread. MRI is particularly useful to determine tumor spread, soft tissue involvement and lymph nodes involvement.
- Electrocardiography
- Blood test: full blood picture and hemoglobin, blood for grouping and cross-matching, urea and electrolytes, and liver function tests.
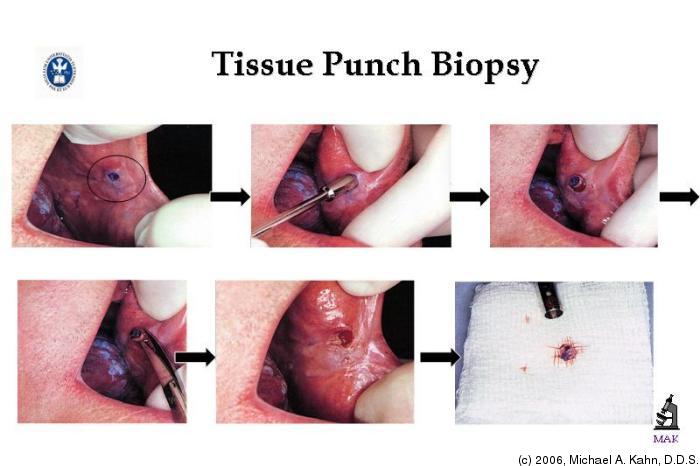
- Biopsy. Biopsy is a tissue sample taken for histopathological analysis and it gives confirmative diagnosis.
© ocw.tufts.edu
In selected cases, other investigations may be indicated:
- Bronchoscopy, if chest x-ray reveals any lesions.
- Endoscopy of the upper aerodigestive tract, especially if there is a history of tobacco use.
- Gastroscopy, if a tube is to be used for feeding.
- Liver ultrasound, if there is enlargement of the liver or abnormal liver function.
- Angiography, in planning lower limb free flaps.
How might you predict the chance of successful treatment?
Prognosis of oral cancer is predicted by using staging and grading. The chances of successful treatment depend on how large the cancer has grown and whether it has already spread to other sites in the body. All cancerous tumors are staged by determining the tumor size (T), the lymph node status (N) and the presence of metastasis (M). These parameters are then combined to give the TNM stage.
Staging of oral cancer
Why is staging done?
- The staging process allows the clinician to have a uniform communicable description of the patient’s disease, for example the extent of cancer
- Helps in treatment plan
- To predict prognosis
- Enables better audit (to compare results within centers)
TNM classification of oral malignancies
© http://dentallecnotes.blogspot.com
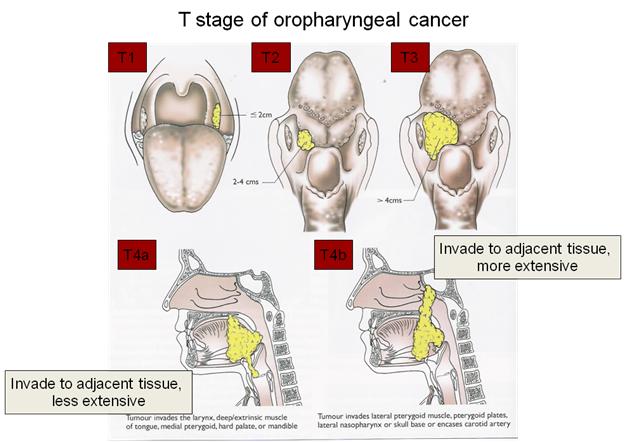
T – Primary tumor
TX – Primary tumor cannot be assessed
T0 – No evidence of primary tumor
TCIS – Carcinoma in situ (a precancerous lesion)
T1 – Tumor 2cm or less in maximum dimension
T2 – Tumor more than 2cm but no more than 4 cm in maximum dimension
T3 – Tumor more than 4cm in maximum dimension
T4 – Tumor invades adjacent structures (bone, muscle, maxillary sinus, skin)
© http://dentallecnotes.blogspot.com
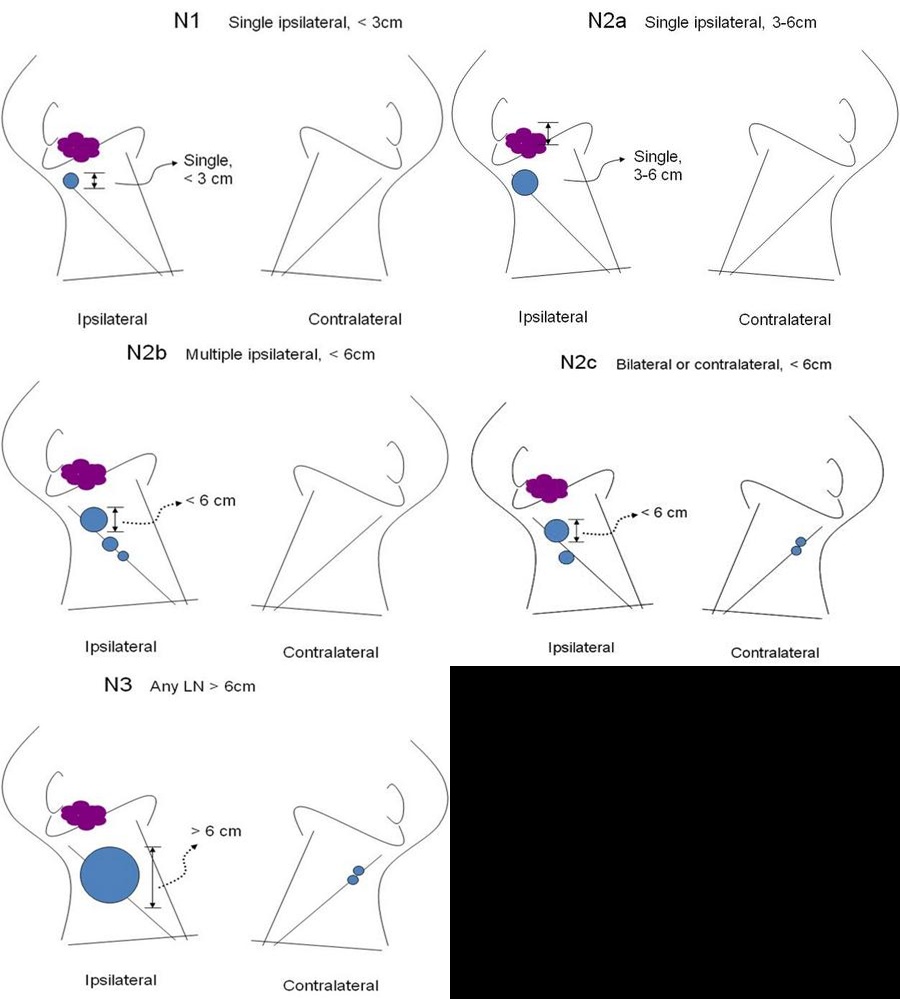
N – Regional lymph nodes
NX – Regional lymph nodes cannot be assessed
N0 – No regional lymph node metastasis
N1 – Metastasis in single ipsilateral (same side) lymph nodes 3cm or less in maximum dimension
N2a – Metastasis in single ipsilateral (same side) lymph nodes more than 3cm but less than 6cm in maximum dimension
N2b – Metastasis in multiple ipsilateral (same side) lymph nodes less than 6cm in maximum dimension
N2c – Metastasis in contralateral (opposite side) or bilateral (both sides) lymph nodes less than 6cm in maximum dimension
N3 – Metastasis in a lymph node more than 6cm in maximum dimension
M – Distant metastasis (spreading of a cancer to another part of the body)
MX – Presence of distant metastasis cannot be assessed
M0 – no distant metastasis
M1 – presence of distant metastasis
Stage grouping of TMN classification
Stage |
T status |
N status |
M status |
Stage 0 |
TCIS | N0 | M0 |
Stage I |
T1 | N0 | M0 |
Stage II |
T2 | N0 | M0 |
Stage III |
T3T1, 2, 3 | N0N1 | M0 |
Stage IV A |
T4T4
T1, 2, 3, 4 |
N0N1
N1,2 |
M0 |
Stage IV B |
T1, 2, 3, 4 | N3 | M0 |
Stage IV C |
T1, 2, 3, 4 | N0, 1, 2, 3 | M1 |
Staging depends on the fact the cancers tend to progress I a predictable way. First they enlarge by invading the surrounding tissues, and then cells break away and travel via the lymphatics to spread in lymph nodes, blood-borne metastases o distant sites develop last. Although sequence is usually predictable, the speed at which any individual cancer progresses through these stages varies widely.
Grading is a histological method to determine how aggressive a cancer is and how quickly it is likely to progress from stage to stage. It is a measure of how differentiated the cancer epithelium is, that is, how much it resembles its tissues of origin. The less it resembles the original tissues, the more aggressive the cancer.
Staging is more important than grading because the size and extent determine whether surgery is possible. Grading is useful in deciding which treatments are appropriate and how radical they should be.
To be continued in Part 5