The neck dissection is a surgical procedure for control of neck lymph node metastasis from Squamous cell carcinoma (SCC) and Merkel cell carcinoma (MCC) of the head and neck. The aim of the procedure is to remove lymph nodes from one side of the neck into which cancer cells may have migrated. Metastasis of squamous cell carcinoma into the lymph nodes of the neck reduce survival and is the most important factor in the spread of the disease. The metastases may originate from SCC of the upper aerodigestive tract, including the oral cavity, tongue, nasopharynx, oropharynx, hypopharynx, and larynx, as well as the thyroid, parotid and posterior scalp.
Division of the Neck into Levels and Sublevels

Lymph nodes in the neck
Memorial Sloan-Kettering Cancer Center developed the lymph node regional definitions most widely used today.
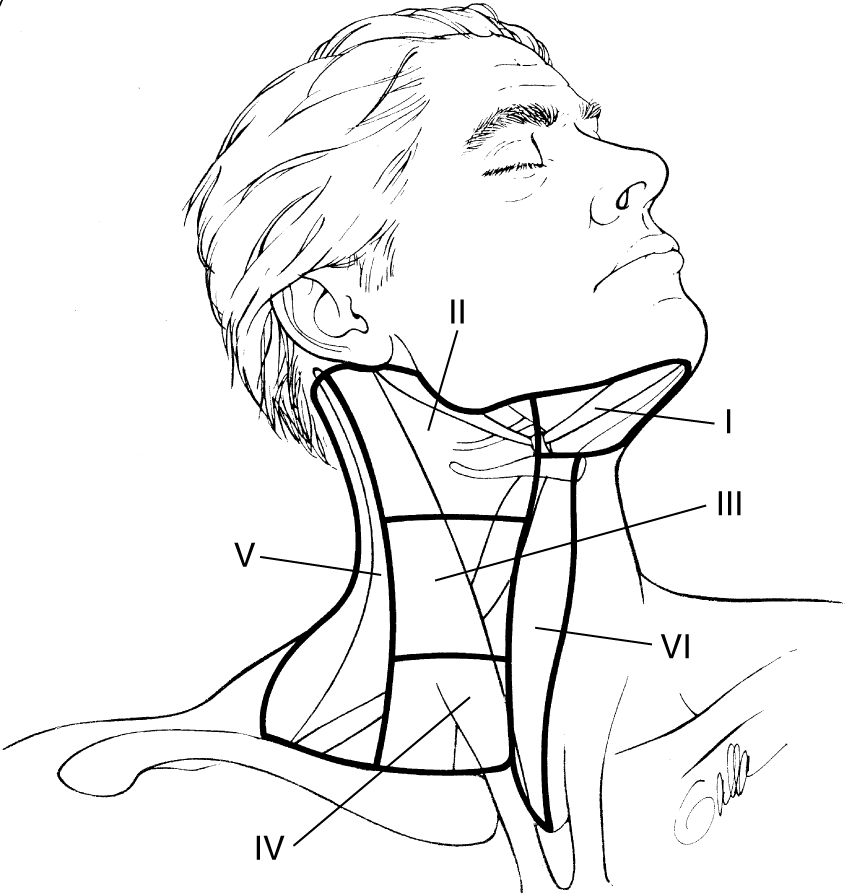
To describe the lymph nodes of the neck for neck dissection, the neck is divided into 6 areas called Levels. The levels are identified by Roman numeral, increasing towards the chest. A further Level VII to denote lymph node groups in the superior mediastinum is no longer used. Instead, lymph nodes in other non-neck regions are referred to by the name of their specific nodal groups.
- Region I: Submental and submandibular triangles. Ia is the submental triangle bound by the anterior bellies of the digastric and the mylohyoid. Ib is the triangle formed by the anterior and posterior bellies of the digastric and body of mandible.
Region II, III, IV: nodes associated with the IJV; fibroadipose tissue located medial to the posterior border of SCM and lateral to the border of the sternohyoid.
- Region II: upper third including the upper jugular and jugulodigastric nodes and the upper posterior cervical nodes. Region bound by the digastric muscle superiorly and the hyoid bone (clinical landmark), or the carotid bifurcation (surgical landmark) inferiorly. IIa contains nodes in the region anterior to the spinal accessory nerve and IIb posterior to the nerve.
- Region III: middle third jugular nodes extending from the carotid bifurcation superiorly to the cricothyroid notch (clinical landmark), or inferior edge of cricoid cartilage (radiological landmark), or omohyoid muscle (surgical landmark).
- Region IV: lower jugular nodes extending from the omohyoid muscle superiorly to the clavicle inferiorly.
- Region V: posterior triangle group of lymph nodes located along the lower half of the spinal accessory nerve and the transverse cervical artery. The supraclavicular nodes are also included in this group. The posterior boundary is the anterior border of the trapezius muscle, the anterior boundary is the posterior border of the sternocleidomastoid muscle, and the inferior boundary is the clavicle.
- Region VI: anterior compartment group comprises lymph nodes surrounding the midline visceral structures of the neck extending from the level of the hyoid bone superiorly to the suprasternal notch inferiorly. On each side, the lateral boundary is the medial border of the carotid sheath. Located within this compartment are the perithyroidal lymph nodes, paratracheal lymph nodes, lymph nodes along the recurrent laryngeal nerves, and precricoid lymph nodes.
 Classification of Neck Dissections
6 levels of lymph nodes in the neck
The 2001 revisions proposed by the American Head and Neck Society (AHNS) and the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) are as follows.
- Radical Neck Dissection (RND) – removal of all ipsilateral cervical lymph node groups from levels I through V, together with SAN, SCM and IJV.
- Modified Radical Neck Dissection (MRND) – removal of all lymph node groups routinely removed in a RND, but with preservation of one or more nonlymphatic structures (SAN, SCM and IJV).
- Selective Neck Dissection (SND) (together with the use of parentheses to denote the levels or sublevels removed) – cervical lymphadenectomy with preservation of one or more lymph node groups that are routinely removed in a RND. Thus for oral cavity cancers, SND (I-III) is commonly performed. For oropharyngeal, hypopharyngeal and laryngeal cancers, SND (II-IV) is the procedure of choice.
- Extended Neck Dissection – This refers to removal of one or more additional lymph node groups or nonlymphatic structures, or both, not encompassed by the RND.
Extent of radical neck dissection
The radical neck dissection is defined as removing all of the lymphatic tissue in regions I-V including removal of the spinal accessory nerve (SAN), sternocleidomastoid muscle (SCM), and internal jugular vein (IJV). It does not include removal of the suboccipital nodes, periparotid nodes except for infraparotid nodes located in the posterior aspect of the submandibular triangle, buccal nodes, retropharyngeal nodes, or paratracheal nodes.
Modified radical neck dissection (MRND) is defined as excision of all lymph nodes routinely removed by radical neck dissection with preservation of one or more nonlymphatic structures, i.e., SAN, IJV, SCM. Medina subclassifies the MRND into types I-III; where type I MRND preserves the SAN, type II MRND preserves the SAN and IJV, and type III MRND preserves the SAN, IJV, and SCM. The type III MRND is also referred to as the “functional neck dissection” as popularized by Bocca, however in his classic description the submandibular gland is not excised.
Selective neck dissection is defined as any type of cervical lymphadenectomy where there is preservation of one or more lymph node groups removed by the radical neck dissection. There are four common subtypes, the first of which is the supraomohyoid neck dissection. This removes lymph tissue contained in regions I-III. The posterior limit of the dissection is marked by the cutaneous branches of the cervical plexus and the posterior border of the SCM. The inferior limit is the superior belly of the omohyoid muscle where it crosses the IJV. The second subtype, posterolateral neck dissection, refers to the removal of the suboccipital lymph nodes, retroauricular lymph nodes, levels II-IV, and level V. This procedure is used most often to remove nodal disease from cutaneous melanoma of the posterior scalp and neck. Originally described by Rochlin in 1962, the SAN, SCM, and IJV were preserved. Medina suggests subclassification of the posteriolateral neck dissection to types I-III to mirror preservation of SAN, IJV, and SCM as in MRND. The lateral neck dissection removes lymph tissue in levels II-IV. Anterior neck dissection is the last subtype of selective neck dissection and refers to the removal of lymph nodes surrounding the visceral structures of the anterior aspect of the neck previously defined as level VI.
The last major subtype is the extended neck dissection defined literally as removal of one or more additional lymph node groups and/or nonlymphatic structures not encompassed by radical neck dissection, such as parapharyngeal, superior mediastinal, and paratracheal. In practice, any of the previous neck dissections may be extended to include other structures. With those definitions in place, the evolution and current indications of the various neck dissections shall be discussed.