Continued from Part 1
© wisdomteeth.com.au
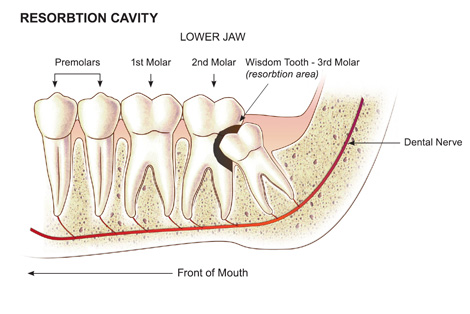
Pressure or mechanical resorption
Root resorption associated with pressure or mechanical stimulation may be seen in individuals undergoing orthodontic treatment and can be caused by the application of excessive force. It occurs in the apical region and the resorbed area undergoes repair and remodeling when the cause is removed. It is possible that excess force could cause an aseptic death of the periodontal ligament, followed by inflammation. Pressure may also be a factor in root resorption associated with tumors or, occasionally, cysts involving the roots of teeth.
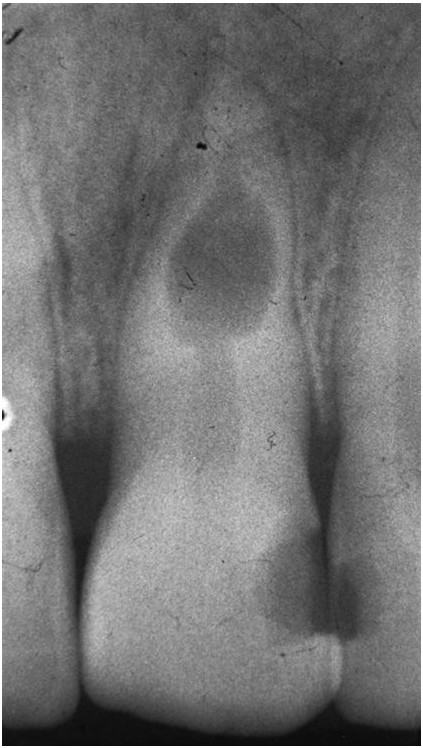
Internal resorption
© quora.com
Internal tooth resorption is less common than external and starts on the pulpal aspect of the dentine. It typically affects the middle third of the root and forms a well-demarcated defect with a smooth symmetrical shape. When the dentine within the crown is involved the resorption may present clinically as a pink spot due to the vascular pulp tissue being visible through the overlying enamel. Internal resorption indicates that the pulp is vital and that, provided the lesion has not perforated the root, the process will be halted by root canal treatment.
What are the tooth resorption causes?
Resorption and repair are physiological processes on the external surface of the root. On the pulpal surface resorption is pathological but repair is one of the pulp’s responses to injury.
External tooth resorption is known to follow damage to the cementum layer or loss of vitality of cementum and this is thought to be why avulsion (total displacement of tooth out of socket) injury is so commonly followed by resorption.
Internal resorption must follow loss of the pre-dentine layer separating the pulp from dentine, but the causes of this loss are unknown. A degree of inflammation or increased pulpal pressure are probably factors.

© drchetan.com
What are the features of tooth resorption?
- Symptomless (unless an inflammatory cause is symptomatic)
- Internal resorption is only active in vital or partially vital teeth
- External resorption may develop on vital or non-vital teeth
- Resorption itself does not compromise vitality of tooth until the pulp communicates with the mouth
- Usually slow and at irregular intervals, occasionally very rapid
- Mobility (loose tooth) or pathological (disease) fracture
- ‘Pink spot’: pulp visible through the crown
- Ankylosis (continuity of tooth and bone)
- Signs of tooth substance loss on x-rays

© softdental.com
What are the signs of tooth ankylosis?
- Lack of normal mobility or movement of tooth
- High pitched metallic percussive sound when tooth is tapped
- Infra occlusion (in the growing jaw): the tooth is below the normal biting line of the mouth
- Sometimes identifiable through x-rays as a bridged periodontal ligament
- Patchy ‘moth-eaten’ root surface or tooth socket lining (lamina dura)
How would tooth resorption be managed in the short and long term?
If the prognosis is poor such as the resorption has involved the periodontal ligament around much of the tooth circumference, the tooth cannot be repaired and it will require extraction. A tooth with a more localized perforation might be repaired surgically. However, in combination with the necessary root canal treatment, this would be a heroic treatment with an unpredictable chance of success. Repair is more likely to be practical for external cervical resorption.
Internal resorption tends to be active in vital or partially vital teeth therefore, provided the lesion has not perforated the root, the process can be halted by root canal treatment.
Time must be given for remodeling of the alveolar or jaw bone before the definitive restoration is made and a temporary replacement will be required.
What are the options for a short-term replacement for tooth resorption?
- Every type or spoon acrylic denture
- Immediate insertion of an adhesive or minimal preparation bridge
- In the very short term, the existing crown might be splinted to the adjacent teeth pending extraction.
What are the options for the long-term replacement for tooth resorption?
Removable partial dentures
Partial dentures are made from acrylic or metal frameworks carrying artificial teeth. These are indicated for individuals with satisfactory oral hygiene and whose remaining teeth have an adequate prognosis, or as in a training/interim appliance prior to full dentures.
Dental bridges
Fixed partial dentures or adhesive bridges are preferable for short empty spans with healthy teeth on either side in well-motivated individuals. A dental bridge is an appliance replacing one or more teeth with artificial teeth fixed unto adjacent natural teeth that cannot be removed by the individual.
Dental implants
Dental implants can be used for single or multiple missing teeth whereby titanium cylinders are painlessly drilled into the jaw bone and artificial teeth or a denture is attached onto it. Dental implants are constructed from a range of materials such as titanium, stainless steel, titanium alloy and zirconium oxide ceramics. However, implants are contraindicated for those having severe illness, pregnant, having uncontrolled metabolic disease (like diabetes) and for those who have improper motivation and unrealistic expectations.