Eruption is the axial movement of a tooth from its nonfunctional position in the bone to functional occlusion. However, eruption is often used to indicate the moment of emergence of the tooth into the oral cavity. The normal eruption of deciduous and permanent teeth into the oral cavity occurs over a broad chronologic age range. Racial, ethnic, sexual, and individual factors can influence eruption and are usually considered in determining the standards of normal eruption. True and significant deviations from accepted norms of eruption time are often observed in clinical practice. Premature eruption has been noted, but delayed tooth eruption (DTE) is the most commonly encountered deviation from normal eruption time.

Erupting teeth
Eruption is a physiologic process that strongly influences the normal development of the craniofacial complex. Often, DTE might be the primary or sole manifestation of local or systemic pathology. A delay in eruption can directly affect the accurate diagnosis, overall treatment planning, and timing of treatment for the orthodontic patient. Thus, DTE can have a significant impact on a patient’s proper health care.
 DEFINITIONS AND TERMINOLOGY
Many terms have been used in the literature to describe disorders of tooth eruption. There seems to be considerable confusion concerning their usage. Eruption is the developmental process responsible for moving a tooth from its crypt position through the alveolar process into the oral cavity to its final position of occlusion with its antagonist. It is a dynamic process that encompasses completion of root development, establishment of the periodontium, and maintenance of a functional occlusion. Emergence, on the other hand, should be reserved for describing the moment of appearance of any part of the cusp or crown through the gingiva. Emergence is synonymous with moment of eruption, which is often used as a clinical marker for eruption.
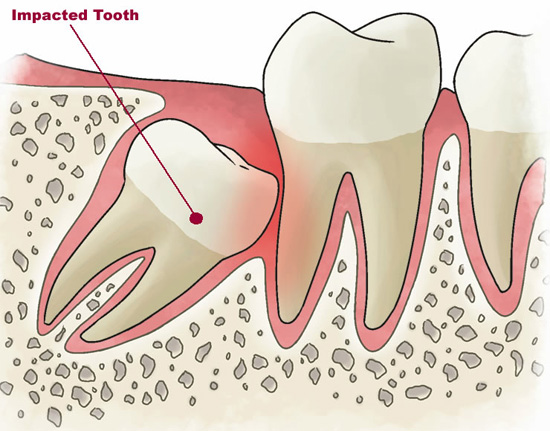 Impacted teeth are those prevented from erupting by some physical barrier in their path. Common factors in the etiology of impacted teeth include lack of space due to crowding of the dental arches or premature loss of deciduous teeth. Frequently, rotation or other positional deviation of tooth buds results in teeth that are “aimed†in the wrong direction, leading to impaction. Primary retention has been used to describe the cessation of eruption of a normally placed and developed tooth germ before emergence, for which no physical barrier can be identified.
Impacted teeth are those prevented from erupting by some physical barrier in their path. Common factors in the etiology of impacted teeth include lack of space due to crowding of the dental arches or premature loss of deciduous teeth. Frequently, rotation or other positional deviation of tooth buds results in teeth that are “aimed†in the wrong direction, leading to impaction. Primary retention has been used to describe the cessation of eruption of a normally placed and developed tooth germ before emergence, for which no physical barrier can be identified.
 Pseudoanodontia is a descriptive term that indicates clinical but not radiographic absence of teeth that should normally be present in the oral cavity for the patient’s dental and chronologic age. In these cases, radiographic examination discloses the teeth in the jaws. These persons might have retained their deciduous teeth; more commonly, the deciduous teeth have been shed, but the permanent ones failed to erupt.
Stages of tooth root development
Controversy exists in the literature about the use of “delayed,†“late,†“retarded,†“depressed,†and “impaired†eruption. Root development has been taken as a basis for distinguishing some of these terms. In 1962, Gron showed that, under normal circumstances, tooth eruption begins when 3/4 of its final root length is established. However, at the moment of eruption, mandibular canines and second molars show more advanced root development than the expected 3/4 of the final root length, whereas mandibular central incisors and first molars show root development less than 3/4 of the expected final root length. Becker suggests that root development alone should be the basis for defining the expected time of eruption for different teeth. Thus, if an erupted tooth has less root development than the expected 3/4 of length, its eruption is deemed premature, whereas if the tooth has developed more than the root length expected for eruption and remains unerupted, it should be defined as having delayed eruption.
Rasmussen and Kotsaki, on the other hand, suggest using established norms for mean eruption ages calculated from population studies. According to them, when the emergence of a tooth is more than 2 standard deviations (SDs) from the mean of established norms for eruption times, it should be considered delayed eruption. However, the authors further propose the terms “late†and “retarded†eruption, to be used on the basis of root development. It would then seem that Rasmussen’s “retarded eruption†coincides with Becker’s and Gron’s “delayed eruption,†and that “late eruption†is used when a tooth’s eruption status is compared with chronologic eruption times defined by population studies.
The terms “depressed†and “impaired†eruption have also been used synonymously with delayed, late, or retarded eruption. However, most of these reports refer to comparisons of observed eruption times with the chronologic standards set by population studies. Thus, “late eruption†used by Rasmussen would describe these conditions best.