
Carious tooth
When caries in your child’s teeth has gone so deep that it has reached, or is near the pulp, your child will need more than just a normal filling to restore the tooth. If the infection from caries has reached the pulp, yet left untreated, the infection may spread causing more harm to your child. The pulp therapy that can be done on your child’s teeth can be divided into vital and non-vital technique:
Vital techniques:
Vital techniques are procedures that attempts to preserve the vitality of the pulp.
1. Indirect pulp cap
Indirect pulp cap is done when caries is judged to be so deep as to be approaching the pulp, such that removal of all caries may result in pulp exposure. Hence, some infected dentine near the pulp is left intact, and a thin layer of calcium hydroxide (CaOH) is placed over the area near to the pulp, and a temporary restoration given, as described in the steps below. This is done in hopes that there’ll be formation of reactionary dentine in response to the CaOH, and a few weeks later, the temporary restoration may be replaced with a permanent one.
Indication:
-when pulpal inflammation is judged to be minimal
-when complete removal of caries will result in pulp exposed
Contraindication:
 -Irreversible pulpitis or any periapical pathology
Procedure:
i) All caries is cleared from the cavity. The softened dentine is gently excavated without exposing the pulp.
ii) A thin layer of Calcium hydroxide (CaOH) is placed on the cavity floor.
iii) The cavity is temporarily filled with zinc oxide eugenol (ZOE, a temporary restoration material).
iv)Â Reinvestigation after 6-8 weeks: remove all softened dentine and restore with a permanent filling.

A thin layer of CaOH placed over exposed pulp (direct pulp capping)
2. Direct pulp cap
This is done when the pulp becomes exposed during removal of caries. A thin layer of CaOH is placed over the exposed pulp area, and the rest of the cavity restored with filling material. However, this procedure is only done in permanent teeth. If done on primary teeth, the CaOH in direct contact with the exposed pulp will cause internal resorption, calcifications or necrosis when it comes in contact with pulp.
Indications:
-no history of spontaneous pain
-no swelling, mobility, discomfort to percussion
-a normal periodontal appearance in x-ray
-pulp tissue should appear vital and normal
-cessation of bleeding from pulp exposure site should occur within 2 minutes
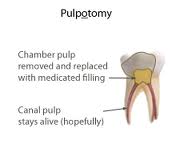
3. Pulpotomy
-This is the complete removal of the infected coronal portion of the dental pulp, followed by placement of a suitable dressing or medicament that will promote healing and preserve vitality of the tooth.
Indications:
i) cariously exposed primary teeth, when their retention is more advantageous than extraction, eg in hemophilic patients.
ii)Â when inflammation is confined to the coronal portion of the pulp.
iii)Â the tooth is free from pulpitis in the root section
iv)Â absence of an abscess or a fistula
Contraindications:
i)Â fistula or swelling,
ii) the tooth crown is nonrestorable,
iii) absent hemorrhage; profuse hemorrhage,
iv) marked tenderness to percussion,
v) mobility,
vi) radiolucency exists in the furcal or periradicular areas,
vii) spontaneous pain, especially at night,
viii) necrotic pulp,
ix) dystrophic calcification (pulp stones).
Technique:
1. Profound anesthesia is given for both tooth and tissue.
2. Isolate the tooth to be treated with a rubber dam.
3. Excavate all caries. If there is no pulp exposure even after all caries is removed, access the pulp chamber from the base of the cavity.
4. Remove the dentin roof of the pulp chamber.
5. Remove all coronal pulp tissue with a slow-speed No. 6 or 8 round bur or sharp spoon excavator.
6. Achieve cessation of bleeding (hemostasis) with dry cotton pellets under pressure.
7. Apply diluted formocresol (or 16% ferric sulfate solution) to pulp on cotton pellet for 3- 5 minutes. Pressure on pellet.

Intermediate restorative material (IRM)
8. Pulp stumps should appear dry.
9. Place a glass ionomer cement (GIC), ZOE, or Intermediate restorative material (IRM) in contact with pulp stumps.
10. Place stainless steel crown (or bonded composite).
Formocresol and its alternative in pulpotomy of Primary Teeth
i) Formocresol: (1) a fixative; (2) chronic inflammation; (3) possibly mutagenic or carcinogenic.
ii) Glutaraldehyde: (1) superior fixation by cross-linkage; (2) diffusibility is limited; (3) excellent antimicrobial agent; (4) causes less necrosis of pulpal tissue; (5) causes less dystrophic calcification in pulp canals; (6) does not stimulate a significant immune response; (7) minimal systemic distribution.
iii) Ferric sulfate: (1) astringent; (2) forms a ferric ion-protein complex that mechanically occludes capillaries; (3) less inflammation than formocresol.
iv)Â Electrosurgery and laser: less successful than ferric sulfate or dilute formocresol.
v) MTA (mineral trioxide aggregate): has regenerative properties, ie it promotes continued growth of the root. This is particularly useful in teeth that has under-developed roots.