
Definition:
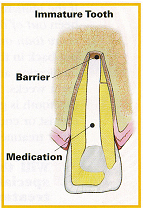
Apexification is a method to induce development of the root apex of an immature, pulp less tooth by formation of osteocementum or other bone-like tissue. It differs from apexogenesis, the physiologic process of root development.
Objective:
The aim of apexification is to induce either closure of the open apical third of the root canal or the formation of an apical “calcific barrier†against which obturation can be achieved.
Rationale:
The technique of treatment is the usual cleaning and irrigation of the root canal, followed by sealing with a paste composed of camphorated chlorophenol and calcium hydroxide.
Radiographic examination is made 3 and 6 months after the procedure, and when evidence of a root apex cap or barrier appears, the root canals are obturated. Actual root growth does not occur as a result of apexification, but radiographic evidence of a calcified mass at the root apex gives that impression.
EXAMINATION: Through pretreatment clinical and radiographic examination.
– symptoms
– swelling
– sinus tract (fistula)
– caries
– history of trauma
– periapical pathosis
INSTRUMENTATION:
Initial working length – radiographic length.
Eliminate seriously infected dentine and soft tissue.
Cannot employ traditional reaming and filing motions.
Over instrumentation to be avoided except in case of acute abscess.
Over instrumentation with larger size instrument is more favorable.
Technique:
1. In apexification procedures every effort should be made to preserve any vital apical pulp tissue that will help the closure of the immature apex.
2. The tooth is anesthetized, the rubber dam is applied, access is gained to the pulp chamber and root canal, and irrigation is performed with sterile water or saline solution. The actual length of the tooth is determined by radiograph.
3. The working length should be at least 2mm short of the length of the tooth. The purpose of cleaning and shaping is to remove any necrotic pulpal tissue and to prepare the root canal for a calcium-hydroxide dressing
4. After thorough cleaning, shaping and irrigation with sterile water or saline solution, the root canal is dried with blunt absorbent points; one must take care not to injure the apical tissues.
5. Calcium hydroxide is mixed with sterile water or anesthetic solution to a thick consistency on a sterile glass slab.
Webber’s technique :
Using amalgam carrier and endodontic pluggers.
Plugger is pre fitted 2-3 mm of radiographic apex and depth marked with a stopper.
3-4 increments of CH is placed with amalgam carries and pushed apicaly with a plugger.
Successive increments is placed with amalgam carrier and pushed apicaly with larger plugger.
Care should be taken to see that calcium hydroxide is in contact with periapical tissue.
ZOE or IRM commonly used.
Calcium hydroxide is vertically condensed to make 4-5 mm of space in access.
Break of occlusal seal leads to, contamination and dilution of paste, also exposure of healing tissues to microorganisms.
6. Barium sulfate can be added to the paste (1 part barium sulfate to 10 parts calcium hydroxide) to increase radiopacity of the mixture. The paste is picked up in an amalgam carrier and is ejected into the pulp chamber.
7. Zinc –phosphate cement is condensed into the access cavity, and the access cavity is sealed with composites.
8. Commercial pastes of calcium hydroxide Ex: Calasept, Pulpdent, Hypo–cal, Calyxl are available in a syringe. A rubber stop is placed on the needle to the working length.
The patient should be recalled for radiograph in 3 months, to determine whether a calcific barrier has developed at or near the root apex; such a barrier denotes that Apexification has occurred.
First at 6 weeks observation visit.
Paste is diluted in canal.
Removed with endodontic instrument of half the diameter of canal.
Reming from the center of canal and dislodging the dry powder.
Subsequently irrigated with saline.
Paste is removed 1-2mm short of the original working length.
Now this is the new working length.
Remaining powder on canal walls removed with larger size instruments.
Canal refilled with new calcium hydroxide paste.
9. If not a fresh supply of calcium-hydroxide paste is applied to the root canal, and the patient is recalled every 3 months until one sees radiographic evidence of an apical barrier denoting apexification.
10. The root canal is obturated after completion of apexification.
Prognosis:
The prognosis for a tooth that has under gone apexification is guarded.
Other Restorative Materials Used in Apexification:
Tricalcium phosphate
Collagen calcium phosphate
Osteogenic protein – 1
Bone growth factors
MTA
Recall :
Recalled 6 wks after second replacement, later 2-3 months there after until calific barrier is formed radiographically.
Total time 12 – 18 months.
Subsequent replacement depends upon radiographic examination.
If any symptoms develop refilling is necessary.