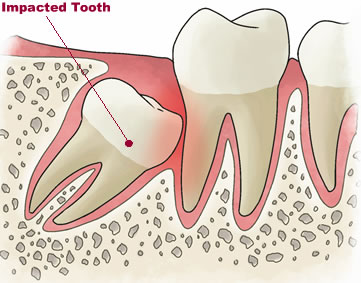
A tooth that is partially erupted or unerupted, beyond the date of eruption is defined as an impacted tooth. Any unerupted tooth can be termed as impacted only when root formation is complete and yet retained in an unerupted position.
Completely Impacted Â
 Â When the tooth is entirely covered by soft tissue and bone, within the bony alveolus, beyond the chronological age of eruption of the particular tooth, even after root apex closure.
 When the tooth is entirely covered by soft tissue and bone, within the bony alveolus, beyond the chronological age of eruption of the particular tooth, even after root apex closure.
Partially EruptedÂ
 Â When the tooth has failed to erpt into a normal functional position but has crossed the bone barrier and has not reached the occusal line.
 When the tooth has failed to erpt into a normal functional position but has crossed the bone barrier and has not reached the occusal line.
Indications For Extraction of Impacted Teeth
- Pericoronitis : This indication will generally exclude “inflammation” that may be associated with the  normal eruption of any tooth. Removal of any asymptomatic impacted tooth should be considered, especially when there have been one or more episodes of infection such as pericoronitis, cellulitis, abscess formation or untreatable pulpal/periapical pathology
- Unrestorable caries : Removal should be considered when there is caries in the impacted tooth and the tooth is unlikely to be usefully restored or when there is caries in the adjacent second molar tooth which cannot be satisfactory treated without removal of 3rd molar.
- Periodontal Disease : Â When there is periodontal disease and pocketing between last/third and second molar, evidence suggests that if removal of third molar is delayed beyond the age of 30 then the condition may become irreversible. Early removal of impacted teeth will result in repair of injured periodontium and is therefore beneficial. Untreated impacted teeth are particularly prone to cause bone loss distal to the adjacent teeth due to pressure effect.
- Third molar removal should be considered in cases of dentigerous cyst formation or other related oral pathology which expands the bone and results in pathological fracture.
- 3rd molar removal should be considered in cases of external resorption of the third molar or second molar where this would appear to be caused by third molar.
- 3rd molar removal may occasionally be indicated for orthodontic or braces reasons
- Removal of 3rd molar may be indicated prior to orthognathic surgery eg:when a sagittal split osteotomy is planned, removal of 3rd molar diminishes the risk of surgical complications with regard to that of osteotomy.
- Prophylactic removal in presence of specific medical and surgical conditions. These include endocardial/valvular scarring/abnormality disposing to bacterial endocarditis, organ transplants, alloplastic implants, chemotherapy/radiotherapy.
- Removal may be considered in cases of fracture of the mandible in the third molar region or when a tooth is involved in tumour resection. The presence of a tooth in a fracture line increases the risk of infection in some cases especially when the tooth has been displaced or rendered non-vital.
- Atypical pain from an unerupted 3rd molar is the most unusual situation and it is essential to avoid any confusion with temperomandibularjoint or muscle dysfunction before considering removal.
- If the third molar tooth is close to the surface or has broken through the surface in relation to an upper or lower denture then it is appropriate to remove that tooth before or as soon as symptoms arise as they are likely to persis and become more severe if the tooth is not removed.
12. 3rd molar removal may be considered for autogenous transplantation to a first molar socket.
Contraindications For Removal of Impaction
- When there is enough space , unerupted teeth should be left in situ to erupt.
- Impacted teeth which are likely erupt successfully and have a functional role in the dentition should not be removed.
- Partially impacted teeth which can be used as an abutment in the construction of fixed partial denture should be left.
- Impacted teeth should not be removed in patients whose medical history renders the removal.
- In patients where the surgical removal of a single third molar tooth is planned under local anesthesia, simultaneous extraction of asymptomatic contralateral teeth should not normally be undertaken.
- Deeply impacted third molars in patients with no history of any bony pathology should not be removed as their removal may cause excessive damage to adjacent structures.
- 3rd molars should not be removed in patients where the risk of surgical complications is judged to be unacceptably high or where fracture of an atrophic mandible may occur.
- Due to socioeconomic reasons , the patient may not be willing to remove the tooth
Classification of Mandibular Teeth Impactions
1) Mesioangular : Impacted tooth is tilted towards the second molar in mesial direction
2) Distoangular : The long axis of the third molar is angled distally posteriorly away from the second molar.
 3) Horizontal : The long axis of the impacted tooth is horizontal
4) Vertical : The long axis of the impacted tooth runs in the same direction as the long axis of the second molar.
Do visit the dentist if you are having pain/discomfort and the dentist will explain and advice a comprehensive treatment for the particular tooth.