The base of the flap should be wider than incisal margins for adequate blood flow to the reflected flap.
The flap should be designed with continuous curvatures between horizontal and vertical incision to avoid sharp angles
5) Incision should be made with firm continuous strokes perpendicular to cortical bone plate.
6) A sinus tract if present should be included
Incision should never be given on bony eminences
A full thickness mucoperiosteal flap should be raised to maintain the integrity of periosteum.
The sutured margins should rest on solid cortical plate.
The two major categories of periradicular surgical flaps are:
Full mucoperiosteal flaps.
Limited mucoperiosteal flaps.
Full mucoperiosteal flaps:
Triangular flap
Trapezoidal flap.
Horizontal (Envelope) flap.
Limited mucoperiosteal flaps:
Submarginal curved flaps (semilunar)
Submarginal rectangular (Leubke – Ochsenbein) flaps.
Full Mucoperiosteal flaps:
In full mucoperiosteal flaps, the entire soft tissue overlying the cortical plate in the surgical site is reflected. This includes the marginal, interdental and attached gingiva, alveolar mucosa, periosteum, and the supra periosteal vessels which supply these tissues.
Advantages:
Blood vessels supplying the tissue remain intact. Rapid wound healing potential
Good surgical access
Minimal untoward post surgical sequelae
Optimal apical orientation.
Disadvantages:
Loss of soft tissue attachment level
Loss of crestal bone height
Post surgical flap dislodgement
Different types of flaps are
Single vertical (Triangular)
Double vertical (Trapezoidal, rectangular)
Scalloped (Leubke ochsenbein)
Curved (semilunar)
Gingival
Minivertical

Triangular Flap:
The single vertical flap is composed of one relaxing vertical incision continuous with horizontal incision along the gingival crest.
Indications:
1. Short roots
2. Radicular repairs
Advantages:
1) Easily modified
2) Visualization of complete length of root
3) Maintains excellent blood supply
4) Easily repositioned
5) Option for performing minor periodontal
surgery.
Disadvantages:
Slight gingival retraction due to crestal bone
resorption and remodeling
Limited access and visibility of long roots.
Double vertical [Trapezoidal/ Rectangular]
Indications:
1) P/A surgery of Multiple teeth
Large lesion
long roots
2) Lateral root perforation repairs
This flap is formed in the same way as triangular with an added oblique incision that results in greater visualization and access to surgical site with less tension.
Advantages:
Provides maximum access and visibility
Reduces retraction tension
Facilitates repositioning
Retro filling of long roots
Disadvantages:
Increased incision and reflection time
Gingival attachment violated
Gingival recession 1-2mm
Suturing difficult
Scalloped [Leukbe-Ochseinbein/sub marginal flap]
It was flap of choice earlier, now it is preferred only in maxillary anteriors where esthetics is of prime concern.
Scalloped or horizontal incision
is in attached gingiva that
parallels free gingival groove.
It is 2mm below muco-gingival
junction or 3mm from free
gingival groove.
Indications:
1) P/A Surgery – in anterior region for
long roots
2) Wide band of attached gingiva is present
Advantages:
Ease in incision and reflection
Greater visibility and access.
Ease in repositioning and suturing into dense
attached gingiva .
Prevents gingival recession
Esthetics is preserved
Disadvantages:
Difficult to alter
Disruption of blood supply
Semi Lunar flap (curved)
Gently curved incision made horizontal in
attached gingiva (curve should be towards the
incisal)
SURGICAL TECHNIQUE
PRE OPERATIVE CONSULTATION
PREMEDICATION-
Drugs should be used to reduce anxiety,bleeding
secondary infection.
1) Anxiety: Phenobarbital, Secobarbital, valium Narcotics.
2) Bleeding: Epinephrine
3) Secondary infection : Antibiotics.
ANAESTHESIA:
Infiltration anesthesia is adequate for maxillary periapical surgery.
Conduction anesthesia is used for mandibular periapical surgery
Additional anesthesia may be used into the medullary bone inside the open wound.
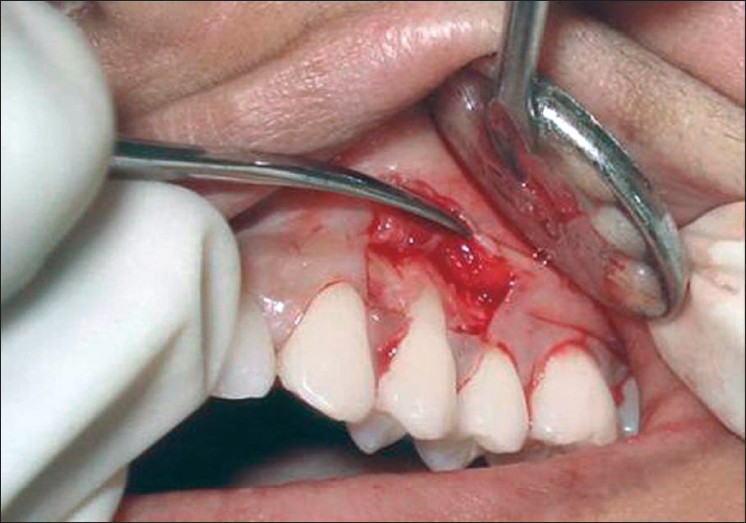
 INCISION-
Is a cut made with a sharp instrument that separates tissue.
With No.15 blade, cut is made through mucosa, connective tissue and periosteum.
Full thickness flap is indicated for periapical surgery.
Any chosen flap should have incision coronal to mucobuccal fold. Never extend into the muscle attachments.
With triangular and trapezoidal flaps, vertical and horizontal incisions should terminate at the line angles of a tooth to preserve integrity of radicular gingival tissue and the papillae.
Elevation and Reflection:
A sharp incision simplifies elevation.
A periosteal elevator separates flap from bone .
Retractors are meant to hold soft tissues away
It may have blunt flat blade or sharp toothed claws.
A solid bone base should be provided to rest the retractor .
Osteotomy:
Helps in uncovering the apex of a diseased tooth. May not be necessary if inflammatory demineralization of bone has already exposed the apex of tooth.
Osteotomy is done with slow speed carbide burs.
Periapical curettage
With the help of a curette
It is inserted into the crypt to cleave the diseased tissues .
Preservation of the tissue in 10% formalin will help conducting of Biopsy.
Root Resection and Retro filling:
Root tip is reduced at a 450 linguolabial level facing the cliniation an retro filling is accomplished.
Debridement of the wound:
Stream of saline / anaesthetic solution is used for irrigation.
Suturing-
A Rg is exposed to verify the proper placement of retrograde filling.
Flap is properly approximated and sutured.