
HYPERTENSION
Hypertension is defined as having
Systolic blood pressure > or = 140mmHg or Diastolic blood pressure > or = to 90mm Hg
1. Essential hypertension.
In more than 95% of cases , no specific underlying cause
2. Secondary hypertension.
In about 5% of cases , hypertension due to specific cause leading to sodium retention and or peripheral vasoconstriction
SYSTOLIC DIASTOLIC
Optimal < 120 < 80
Normal < 130 < 85 High normal 130-139 85-89 Stage 1 (HPN) 140-159 90-99 Stage 2 160-179 100-109 Stage 3 > 180 > 110
APPROACH TO DIAGNOSIS
1. Accurate measurements of BP
2. Identify any underlying hypertension
3. Recognize other risk factors for the development of CVS diseases.
4. To detect any complication (target organ damage).
INVESTIGATIONS
Urinalysis, Serum Na, K,
Plasma urea /creatinine
Plasma cholesterol
Chest radiograph
ECG
Echo in selected cases.
MANAGEMENT
General measures:
Weight reduction, Exercise, Moderation of alcohol, Decrease intake of Na, increase intake of Ca and K, Stop smoking.
Relaxation techniques.
DRUG TREATMENT
1. Thiazide diuretics : first line treatment especially in elderly patients.
2. Beta – adrenoreceptor antagonist :can be used in combination with a thiazide .
3. Calcium antagonist :where beta – adrenoreceptor antagonist contraindicated or not tolerated
4. ACE- inhibitors :used when first line of treatment fails , most effective in combination with thiazide
5. Aspirin : indicated to reduce cardiac and stroke complications
DENTAL CONSIDERATIONS
Bleeding – untreated/ uncontrolled hypertension
Drug Side effects:
β Blocker – Xerostomia lichenoid reaction.
ACE inhibitor – burning mouth, scalded mouth syndrome, loss of taste
Calcium channel blocker – gingival hyperplasia
Diuretics electrolyte imbalance
frusemide – hypokalaemia
DENTAL MANAGEMENT
Anxiety associated with dental treatment causes increase in BP. Preoperative reassurance and sedation .
Early morning appointments of short duration
Adequate anesthesia /analgesia .
Long term NSAIDS are best avoided.
Patients with hypertension can be treated with adrenaline in the ratio of 1:80,000.
If patient complains of postural giddiness, do NOT elevate the patient suddenly from supine to upright position.
INFECTIVE ENDOCARDITIS
Definition
Infection of valvular or mural endocardium.
Aetiology
Infective endocarditis is due to microbial infection of a heart valve (native or prosthetic), the lining of a cardiac chambers or blood vessels, or a congenital anomaly (septal defect).
UNDERLYING HEART DISEASES:
Fever in a patient with known heart disease.
Change in heart murmurs or appearance of new murmurs.
Recent deterioration in cardiac status.
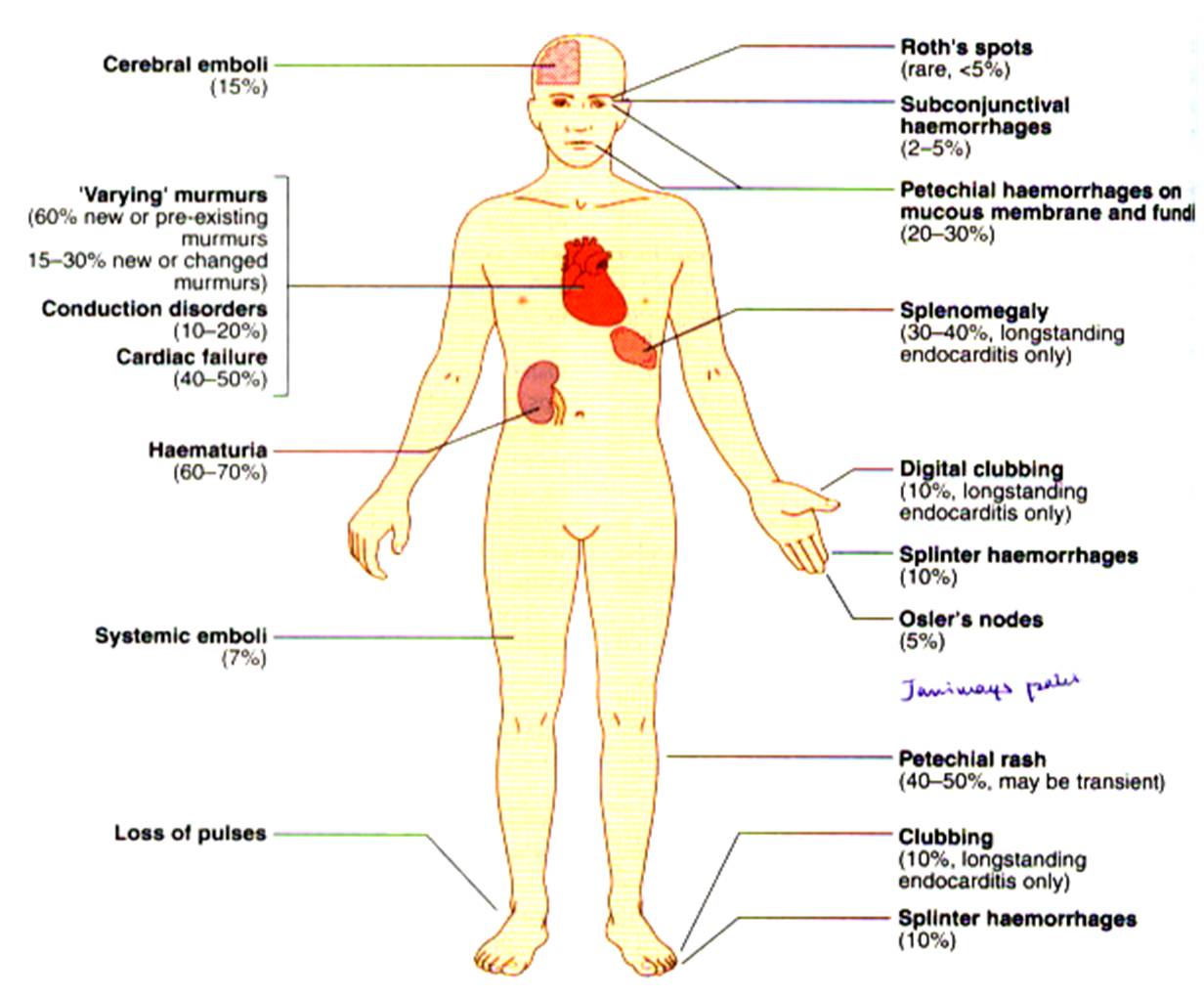
Clubbing, splinter hemorrhages, Janeway’s lesions, Osler’s nodes, splenomegaly, Roth’s spots, hematuria, absent peripheral pulses.
Rheumatic valvular diseases 30%
Congenital heart diseases 10-20%.
Mitral valve prolapse 10-33%.
Degenerative heart diseases- calcific AS, syphilitic AR, Marfan’s syndrome, AV fistula.
No underlying heart disease in 20-40%.
CLINICAL FEATURES
Fever in a patient with known heart disease.
Change in heart murmurs or appearance of new murmurs.
Recent deterioration in cardiac status.
Clubbing, splinter hemorrhages, Janeway’s lesions, Osler’s nodes, splenomegaly, Roth’s spots, hematuria, absent peripheral pulses.
INVESTIGATIONS
Blood culture – 3 Samples, 20 ml, 1/2 hr interval
2 D – Echocardiography.
ECG
Measurement of plasma C-reactive protein
Raised ESR
Chest radiograph .
TREATMENT
High dose antibiotics, i.v route, given for 4-6 weeks
Benzyl Penicillin / Cefazolin / Vancomycin
Gentamycin / Tobramycin / Amikacin.
Tetracycline for Rickettsiae and Chlamydiae.
Amphotericin B for fungal infections.
PREVENTION
Patients with valvular or congenital heart disease may be susceptible to infective endocarditis.
Patient should be aware of the risk of endocarditis, the need to avoid bacteremia
Potential sources of infection should be treated promptly.
CARDIAC CONDITIONS ASSOCIATED WITH ENDOCARDITIS
ENDOCARDITIS PROPHYLAXIS RECOMMENDED
Prosthetic heart valves (bioprosthetic or homograft valve)
Previous bacterial endocarditis
Complex cyanotic congenital heart disease (eg: single ventricle states)
ENDOCARDITIS PROPHYLAXIS NOT RECOMMENDED
Isolated secundum atrial septal defect
Surgical repair of ASD, VSD, or PDA (without residue beyond 6 month)
Previous coronary artery bypass graft surgery performed more than 6 weeks prior to treatment
Mitral valve prolapse without valvular regurgitation
Physiologic, functional, or innocent heart murmurs
Previous Kawasaki disease or rheumatic fever without valvular dysfunction
Cardiac pacemakers and implanted defibrillators
STANDARD REGIMENS FOR ANTIBIOTIC
PROPHYLAXIS MINIMIZE RISK OF ENDOCARDITIS
AFTER ORAL PROOCEDURES
ADULTS, NOT ALLERGIC TO PENICILLIN
2.0 g Amoxicillin 1 h before procedure
2.0g Ampicillin IM or IV within 30 min before procedure
ADULTS, PENICILLIN ALLERGIC
600 mg Clindamycin 1 h before procedure or
2.0g Cephalexin 1 hour before procedure
or
500mg Azithromycin or Clarithromycin 1hr before procedure
600mg Clindamycin IV within 30 min before procedure
or
1.0g Cefazolin IM or IV within 30 min before procedure
CHILDREN, NOT ALLERGIC TO PENICILLIN
50 mg/kg Amoxicillin 1 h before procedures
50 mg/kg Ampicillin IM or IV within 30 min before procedures
CHILDREN, PENICILLIN ALLERGIC
20 mg/kg Clindamycin 1 h before procedure
or
50 mg/kg Cephalexin or cefadroxil 1 h before procedure
or
15 mg/kg Azithromycin
or
Clarithromycin 1 h before procedure
20 mg/kg IV Clindamycin within 30 min prior to procedure
or
25 mg/kg IM or IV Cefazolin 30 min before procedure
Oral procedures requiring antibiotic prophylaxis
Extractions
Periodontal procedures including surgery, subgingival placements of antibiotic fibers or strips, scaling, and root planning
Implant placement
Tooth reimplantation
Placement of orthodontic bands (not brackets)
Endodontic instrumentation (beyond the apex) or surgery
lntraligamentary injections
Prophylactic cleaning of teeth where bleeding is anticipated
Other procedures in which significant bleeding is anticipated
Oral Procedures Not Requiring Prophylaxis
Operative and prosthodontic procedures with or without retraction cord (including restoration of decayed teeth and replacement of missing teeth)
Local anesthetic injections (non intraligamentary)
Intracanal endodontic procedures (including post placement and buildup)
Placement of removable prosthodontic or orthodontic appliances
Orthodontic appliance adjustment
Impression making
Exfoliation of primary teeth
Oral radiography
Fluoride treatments
Placement of rubber dams
Postoperative suture removal