Multiple myeloma (from Greek myelo-, bone marrow), also known as plasma cell myeloma or Kahler’s disease (after Otto Kahler), is cancer of the plasma cells in bone marrow.
Causes, incidence, and risk factors
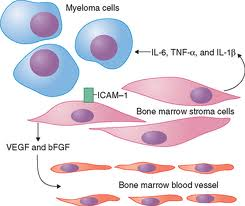 Plasma cells help your body fight infection by producing proteins called antibodies. In multiple myeloma, plasma cells grow out of control in the bone marrow and form tumors in the areas of solid bone.
Plasma cells help your body fight infection by producing proteins called antibodies. In multiple myeloma, plasma cells grow out of control in the bone marrow and form tumors in the areas of solid bone.
The growth of these bone tumors makes it harder for the bone marrow to make healthy blood cells and platelets.
Multiple myeloma mainly affects older adults. Past treatment with radiation therapy raises your risk for this type of cancer.
Symptoms
Multiple myeloma causes anemia, which makes a person more likely to get infections and have abnormal bleeding.
As the cancer cells grow in the bone marrow, bone or back pain, most often in the ribs or back.
If the bones in the spine are affected, it can put pressure on the nerves, resulting in numbness or weakness of the arms or legs.
Other symptoms include:
- Bleeding problems
- Fatigue due to anemia
- Fevers without any other cause
- Shortness of breath due to anemia
- Unexplained broken bones
Signs and tests
 Blood tests can help diagnose this disease. They may include:
Blood tests can help diagnose this disease. They may include:
- Blood tests to check calcium level, total protein level, and kidney function
- Complete blood count (CBC)
- Blood and urine tests to check to identify proteins, or antibodies (immunofixation)
- Blood tests to quickly and accurately measure the specific level of certain proteins called immunoglobulins (nephelometry)
This list is not all-inclusive.
Bone x-rays may show fractures or hollowed out areas of bone. If your doctor suspects this type of cancer, a bone marrow biopsy will be performed.
Bone density testing may show bone loss.
Treatment
The goal of treatment is to relieve symptoms, avoid complications, and prolong life.
People who have mild disease or where the diagnosis is not certain are usually carefully watched without treatment. Some people have a slow-developing form of multiple myeloma that takes years to cause symptoms.
Medications for the treatment of multiple myeloma include:
- Dexamethasone, melphalan, cyclophosphamide, doxil, thalidomide, lenalidomide (Revlimid), and bortezomib (Velcade) can be used alone or combined together.
- Bisphosphonates (pamidronate) to reduce bone pain and prevent fractures.
Radiation therapy may be done to relieve bone pain or treat a bone tumor.
Two types of bone marrow transplantation may be tried:
- Autologous bone marrow or stem cell transplantation makes use of one’s own stem cells. In younger patients, it has been shown to increase survival.
- Allogeneic transplant makes use of someone else’s stem cells. This treatment carries serious risks but offers the chance of a cure.
People with multiple myeloma should drink plenty of fluids to prevent dehydration and help maintain proper kidney function. They should also be cautious when having x-ray tests that use contrast dye.
Dental relevance

Osteoradionecrosis dur to treatment from multiple myeloma
Approximately 5 to 30% of myeloma patients have lesions in the jaw. Incidental discovery of lesions in the jaw may be the first evidence of this disease. Although uncommon, an initial presentation of multiple myeloma may reveal oral or maxillofacial symptoms. The oral manifestations of MM are the first sign of the disease in about 14% of the patients.
The patient may experience pain, swelling, numbness of the jaws, epulis formation, or unexplained mobility of the teeth.
More than 30% of patients with MM develop osteolytic lesions in the jaw. Osteolytic lesions are more frequent in the mandible than in the maxilla, especially in the posterior teeth region, ramus and condylar process, presumably because of greater hematopoietic activity in these areas. The radiographic appearance of the lesions is generally punched out osteolytic lesions (60%). In most instances, the lesions appear unassociated with the apices of the teeth. From the radiological point of view, MM can exhibit three distinct radiographic aspects in the skeletal system, including, in the maxillaries:
1. Bone with no apparent alteration
2. Multiple radiolucent areas
3. Generalized bone rarefaction
4. Osteoporotic alterations
There is also the problem of jaw osteonecrosis following prolonged use of bisphosphonates such as Aredia (pamidronate) and Zometa (zoledronic acid). This has been widely reported since 2003 and indeed mentioned in two recent editions of this journal. These drugs are routinely administered by monthly infusion to myeloma patients to prevent bone damage but may trigger problems with bone healing in a small subset of patients following dental surgery. This includes tooth extraction, endodontics and periodontal treatment. Close cooperation is required with the patient’s haematologist in these circumstances and it may be advisable to stop the bisphosphonates for three months before any treatment.
Support Groups
The stress of illness may be eased by joining a support group whose members share common experiences and problems.
Expectations (prognosis)
Survival of people with multiple myeloma depends on the patient’s age and the stage of disease. Some cases are very aggressive, while others take years to get worse.
Chemotherapy and transplants rarely lead to a permanent cure.
Complications
 Kidney failure is a frequent complication. Other complications may include:
Kidney failure is a frequent complication. Other complications may include:
- Bone fractures
- High levels of calcium in the blood, which can be very dangerous
- Increased chances for infection (especially pneumonia)
- Paralysis from tumor or spinal cord compression
Calling your health care provider
Call your doctor if you have multiple myeloma and infection develops, or numbness, loss of movement, or loss of sensation develops.