- Complex facial fractures: Such fractures can be reconstructed best after open reduction and fixation of the mandibular segments to provide a stable base for restoration.
- Condylar fractures: Although strong evidence supporting open reduction of condylar fractures is lacking, a specific group of individuals benefit from surgical intervention. The classic article by Zide and Kent lists absolute and relative indications for open reduction of the fractured mandibular condyle.Palmieri et aland De Riu et aldemonstrated better long-term range of motion and occlusion in patients with condylar factures treated with ORIF versus closed reduction and MMF.
- Absolute indications
- Displacement of the condyle into the middle cranial fossa
- Inability to obtain adequate occlusion by closed techniques
- Lateral extracapsular dislocation of the condyle
- Relative indications
- Bilateral condylar fractures in an edentulous patient when splints are unavailable or impossible because of severe ridge atrophy
- Unilateral or bilateral condylar fractures when splinting is not recommended because of concomitant medical conditions or when physiotherapy is not possible
- Bilateral fractures associated with comminuted midfacial fractures
- Mandibular nonunions require open access for debridement and subsequent reduction.
- Malunions after improper reduction often require osteotomies through open surgical approaches to correct mandibular discrepancies.
Timing of open reduction
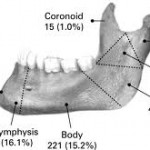
Percentages of mandibular fractures happening at each location
Traditional teaching has been that mandible fractures should be reduced within 24 hours of injury.Recent studies have shown no increase in complications with a delay of repair beyond 24 hours.Biller et al showed no increase in infections in repairs delayed over 72 hours, but there was an increased incidence of technical complications.Barker et al showed no correlation of complications and delay of repair of over 2 weeks.
Contraindications
Contraindications to closed reduction include the following (these patients benefit from open reduction and rigid internal fixation [ORIF]):
- Patients with poorly controlled seizure history
- Patients with compromised pulmonary function (ie, moderate-to-severe asthma, chronic obstructive pulmonary disease)
- Patients with psychiatric or neurologic problems
- Patients with eating or GI disorders
Epidemiology
Frequency
Numerous investigators have reported studies on populations on all continents; fractures of the mandible have been reported to account for 36-70% of all maxillofacial fractures.All reports apparently show a higher frequency in males aged 21-30 y.Other contributing factors, such as socioeconomic status, environment, alcohol use, and mechanisms, show greater variability.
Etiology
 Major etiologic factors vary based on geographic location. Investigators in countries such as Jordan, Singapore, Nigeria, New Zealand, Denmark, Greece,and Japan reported motor vehicle accidents to be the most common cause; in reports from other countries such as Greenland, Finland, Scotland, Sweden, Bulgaria, and Canada found assaults to be the most common etiology.
Major etiologic factors vary based on geographic location. Investigators in countries such as Jordan, Singapore, Nigeria, New Zealand, Denmark, Greece,and Japan reported motor vehicle accidents to be the most common cause; in reports from other countries such as Greenland, Finland, Scotland, Sweden, Bulgaria, and Canada found assaults to be the most common etiology.
Results in the United States have been divided. In 1982, Olson and associates demonstrated that vehicular accidents caused 48% of fractures.In 1985, Fridrich and associates demonstrated that altercations accounted for 47% of fractures and automobile accidents for 27%. Also in 1985, Ellis et al reported that 43% were caused by vehicular accidents, 34% were caused by assaults, 7% were work-related, 7% occurred as the result of a fall, 4% occurred in sporting accidents, and the remainder had miscellaneous causes.
Vaillant and Benoist described 14 cases of gunshot injuries to the mandible; 2 children had injuries that resulted from accidents, and the adults’ fractures were caused by suicide or assault.
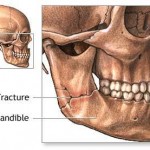
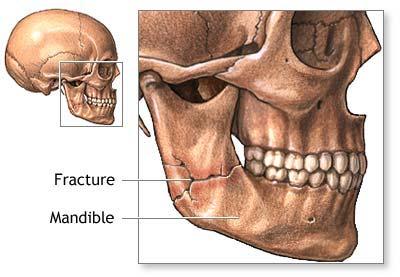
Location of mandibular fractures
Fridrich and associates showed that most fractures occur in the body (29%), condyle (26%), and angle (25%) of the mandible. The symphyses account for 17% of mandibular fractures, whereas fractures of the ramus (4%) and coronoid process (1%) have lower occurrence rates. In automobile accidents, the condylar region was the most common fractured site. In motorcycle accidents, the symphysis was fractured most often. When assault was the cause, the angle demonstrated the highest incidence of fracture.
Associated injuries with mandibular fractures
Fridrich and associates reported that in patients with mandible fractures, 43% of the patients had an associated injury. Of these patients, head injuries occurred in 39% of patients, head and neck lacerations in 30%, midface fractures in 28%, ocular injuries in 16%, nasal fractures in 12%, and cervical spine fractures in 11%. Other injuries present in this group were extremity trauma in 51%, thoracic trauma in 29%, and abdominal trauma in 14%. Of the 1067 patients studied, 12 (2.6%) died of their associated injuries before the mandible fracture could be treated.
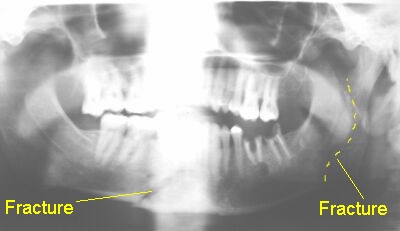
Number of fractures per mandible
In patients with mandible fractures, 53% of patients had unilateral fractures, 37% of the patients had 2 fractures, and 9% had 3 or more fractures.
Presentation
History
- A complete medical and psychiatric history is important for diagnosis and future treatment of mandible fractures.
- Thoroughly explore possible bleeding disorders, endocrine disorders, or bony and collagenous disorders prior to surgery.
- History of previous mandibular trauma can help prevent misdiagnoses.
- Any pretraumatic temporomandibular joint dysfunction needs to be documented in detail prior to treatment.
- The source, size, and direction of traumatic force are helpful in diagnosis.
- Fractures sustained by a fist tend to have single, simple, or nondisplaced fractures whereas patients involved in motor vehicle accidents sustain compound comminuted fractures.
- Localized trauma (eg, pipe, stick, hammer) tends to cause a single comminuted fracture since the force is concentrated in a small area.
- Trauma distributed to a larger surface area may cause several fractures (eg, symphysis, condyle) secondary to distribution of the force throughout the mandible.
- Direction of the force can help in making the diagnosis of concomitant fractures. Trauma directed to the chin often results in a symphyseal fracture with concomitant unilateral or bilateral condylar fractures.