The resin bonded bridge is primarily used for your front teeth. Less expensive, this bridge is best used when the abutment teeth are healthy and don’t have large fillings. The false tooth is fused to metal bands that are bonded to the abutment teeth with a resin which is hidden from view. This type of bridge reduces the amount of preparation on the adjacent teeth.
 A bonded bridge, also called a Maryland bridge, is a great way to replace a missing tooth when used in the right situation. A bonded bridge is comprised of one or two artificial teeth with “wings” connected on each side. To replace a tooth, the wings are fastened to the inside of a person’s teeth on either side of the missing one.
A bonded bridge, also called a Maryland bridge, is a great way to replace a missing tooth when used in the right situation. A bonded bridge is comprised of one or two artificial teeth with “wings” connected on each side. To replace a tooth, the wings are fastened to the inside of a person’s teeth on either side of the missing one.
In recent years, the bonded bridge has fallen out of favor with many dentists because the wings, previously made only out of metal, were unaesthetic, and would require frequent visits to refasten it. Today, the bonded bridge wings can be made out of durable resin materials that are both cosmetically pleasing, and attach firmly to the teeth.
The wing or retainer must be rigid and is usually fabricated from a metal alloy. The inner surface must fit closely to the abutment tooth. The intaglio is treated in some way to enhance the micromechanical adhesion between the prosthesis and the composite resin cement. In the past various methods have been used, ranging from metal-weave patterns to tin plating. The modern resin retained bridge retaining wing is usually sandblasted with an alumina powder.
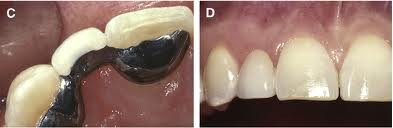
C. When view from the palate D. When view from outside of the mouth
The pontic is usually made from dental porcelain. The whole restoration is thus a porcelain fused to metal restoration.
Current cement brands commonly used for this procedure include Panavia, Nexus. All are either auto cure or dual cure to ensure complete polymerisation of the resin under the wing. Great care must be taken during cementation to avoid contamination of the operative field as this will lower the bond strength of the cement and lead to premature failure. For this reason rubber dam is often advocated for placement, though this can bring its own difficulties.
One common way to use the bonded bridge is when someone comes to the office with a loose tooth in the front of his or her mouth that cannot be saved. The adjacent teeth are gently prepared for the bonded bridge, and then take a mold (impression).
Next, the impression will be sent to the lab that makes the bonded bridge. The patient is brought back to remove the loose tooth and put in place the bonded bridge on the same visit. This way, the patient is rid of the unsavable tooth and never has to go without a tooth in the front of his or her mouth. Another advantage of the bonded bridge is that the wings can help stabilize the teeth that they are fastened to. This is especially important when the teeth are slightly loose due to periodontal (gum) disease.
 The bonded bridge has several benefits over conventional fixed bridgework (a series of joined caps or crowns). These benefits include reduced cost, less drilling or preparation of the teeth, and less time required to complete the treatment. As dentine preparation is not involved, the integrity of a young pulp is maintained. Other advantages include the fact that anaesthesia is not normally required, soft tissues are not disturbed which simplifies impression procedures, and margins are supragingival, facilitating plaque removal. A failure rarely results in any adverse long-term consequences for the patient unless periodontal or orthodontic splinting has been employed.
The bonded bridge has several benefits over conventional fixed bridgework (a series of joined caps or crowns). These benefits include reduced cost, less drilling or preparation of the teeth, and less time required to complete the treatment. As dentine preparation is not involved, the integrity of a young pulp is maintained. Other advantages include the fact that anaesthesia is not normally required, soft tissues are not disturbed which simplifies impression procedures, and margins are supragingival, facilitating plaque removal. A failure rarely results in any adverse long-term consequences for the patient unless periodontal or orthodontic splinting has been employed.
Despite these benefits, there are some drawbacks. The bonded bridge is not as strong as fixed bridgework, and is generally only appropriate in the front of the mouth where biting forces are typically not strong. Aesthetics may be compromised by ‘shine through’ of metal retainers, resulting in discoloration of the abutment teeth. This situation can be improved with the use of opaque luting cement but this can, in turn, result in a loss of translucency and a highly visible white line if used where there is incisal coverage. Although it is possible to assess the appearance of the bridge with ‘try in’ pastes prior to cementation, there is no trial phase to test any occlusal changes. Generally, tooth movement will occur within six to nine months if the bridge is fitted ‘high’.
The decision to use a bonded bridge is at the discretion of your dentist. People with heavy jaw musculature, have weak or very loose teeth, those who grind their teeth during the day or at night, or have too large a space where the teeth are missing may not be good candidates for the procedure. Even so, in some cases, a bonded bridge might be the best way to replace a missing tooth.