Trauma exerted onto the head and neck region can cause a fracture to any of the bones. The lower jaw, or the mandible, is particularly prone to fracture. In this article we will discuss some of the aspects related to fracture of the lower jaw (mandibular fracture).
CAUSES OF JAW FRACTURE (upper or lower):
- Accidents: Motor-vehicle accidents (MVA), sports injuries, occupational (accidents that occur during work)
- Falls (eg, falling down the stairs, slipping on a slippery floor)
- Assault and fights
- Pathological– a pathology such as tumours or cysts in the jaw bone can cause thinning of the bone or decrease in density of the bone, ultimately leading to fracture of bone in that region, even when a light external force is applied to the bone.
CLASSIFICATION OF MANDIBULAR FRACTURE
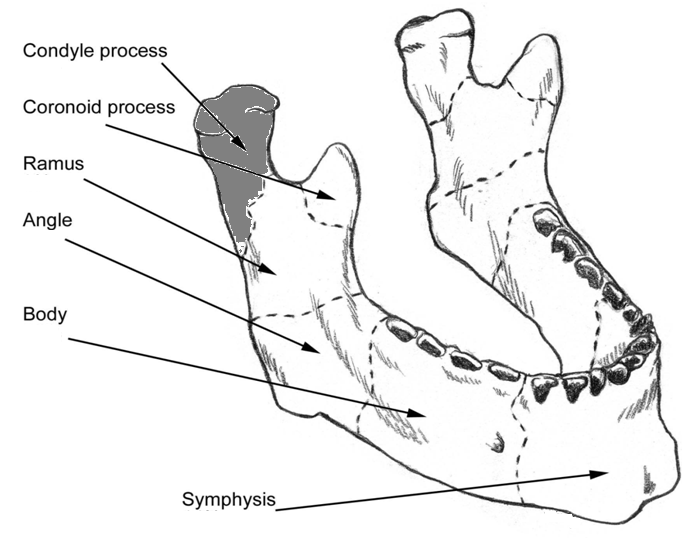
1. by anatomic location
- Condyle
- Coronoid  process
- Ramus
- Angle
- Parasymphysis/body
- Symphysis
The most commonly affected sites are the condyle process, the angle of the mandible, and the parasymphysis region, particularly in the region where the canine tooth is, for the following reasons:
i) Condyle process: the condyle process has a thin neck and thus is susceptible to fracture. Fracture can occur on both right and left side (bilateral condyle fracture) or just on any one side (unilateral fracture). Bilateral fracture is usually due to a blow to the chin from the front, particularly when the mouth is open. Unilateral fracture is usually due to a blow from the opposite side of the face, along with fracture of the parasymphysis on the side of the blow. Eg a blow to the jaw from the right side will result in right parasymphysis fracture and left condylar fracture.

Boomerang
ii) Angle of the mandible: this site is a weak point due to the following reasons:
- the angle of the mandible is the junction where there is a change of direction in bone, i.e. the horizontal part of the jaw meets the vertical part of the jaw. Just like a boomerang, when excessive force is applied onto the boomerang, it tends to break in the middle where the two ends meet.
- this part of the mandible becomes thin in cross section as compared to its adjacent parts
- This is where the wisdom tooth grows, and an unerupted wisdom tooth occupies two thirds of the depth of the bone, which makes the bone weak in this region.
iii) Parasymphysis in the region of canine tooth: the canine tooth has the longest root compared to other teeth, hence along the long axis of the tooth socket, there is relatively less bone, thus creating a weak point in the jaw.
2. by type of fracture
- Simple/closed– the fracture of the bone is not continuous with the skin or oral tissues, i.e. not exposed to the external environment.
- Compound-the fracture is exposed to the external environment.
- Comminuted– the bone is broken into small pieces, as though it was crushed.
- Complicated– vital structures are involved along with the bone injury, such as nerve bundles, blood vessels or the middle cranial fossa
- Greenstick– an incomplete fracture whereby one side of the bone is broken, while the other side is intact, making the bone appear bent, like a young and green twig, thus the name. This is more common in young children, as the bone is not fully developed.
- Pathological-as explained above, fracture is caused by a pre-existing bone pathology causing weakness in the bone.
Radiologic Evaluation

Example of an OPG
Often clinical visualization can be limited by the soft tissues and bleeding or swelling that follows trauma. Thus it is essential to have radiological aids for proper evaluation of the fracture:
- CT Scans
- X-rays:
–Orthopantomograph (OPG): especially useful in visualizing fractures in the teeth-bearing area
–Occipitomental view (OM)– useful for fractures of the middle 3rd of face and coronoid process
–PA skull (posterior-anterior view)-gives a general view of the head
–Submentovertex view– gives a good view of the zygomaticomaxillary complex(zmc), i.e. the cheekbone
-Reverse Towne’s projection- ideal for seeing condylar fractures
PRINCIPLES OF MANAGEMENT OFÂ JAW FRACTURES:
 If you had a pair of eye glasses that has broken in half and you want to fix it back, you would do it by approximating the two halves into its original position (reduction), gluing it together, eg by using superglue or tape (fixation), and setting it aside untouched for a period of time to allow the superglue to set and bond the 2 halves together (immobilization). The same principle applies to bone fracture; you would want to:
If you had a pair of eye glasses that has broken in half and you want to fix it back, you would do it by approximating the two halves into its original position (reduction), gluing it together, eg by using superglue or tape (fixation), and setting it aside untouched for a period of time to allow the superglue to set and bond the 2 halves together (immobilization). The same principle applies to bone fracture; you would want to:
- Reduce the fracture
- Fix & stabilize the fracture
- Immobilization of fracture segments for a period of time to allow healing of bone
- Restore the occlusion (how the patient bite together) to its original position
- Prevent/ eradicate infection in fracture site