Mucosal barrier has also been suggested as an etiologic factor in DTE. Any failure of the follicle of an erupting tooth to unite with the mucosa will entail a delay in the breakdown of the mucosa and constitute a barrier to emergence. Histologic studies have shown differences in the submucosa between normal tissues and tissues with a history of trauma or surgery. Gingival hyperplasia resulting from various causes (hormonal or hereditary causes, vitamin C deficiency, drugs such as phenytoin) might cause an abundance of dense connective tissue or acellular collagen that can be an impediment to tooth eruption.
Injury to primary teeth
Injuries to deciduous teeth have also been implicated as a cause of DTE of the permanent teeth. Smith and Rapp, in a cephalometric study of the developmental relationship between deciduous and permanent maxillary central incisors, found that the bony tissue barrier between the deciduous incisor and its successor has a thickness of less than 3 mm. This intimate relationship between the permanent and deciduous incisors is maintained during the developmental years. Traumatic injuries can lead to ectopic eruption or some disruption in normal odontogenesis in the form of dilacerations or physical displacement of the permanent germ. Cystic transformation of a nonvital deciduous incisor might also cause delay in the eruption of the permanent successor. In some instances, the traumatized deciduous incisor might become ankylosed or delayed in its root resorption. This also leads to the overretention of the deciduous tooth and disruption in the eruption of its successor.
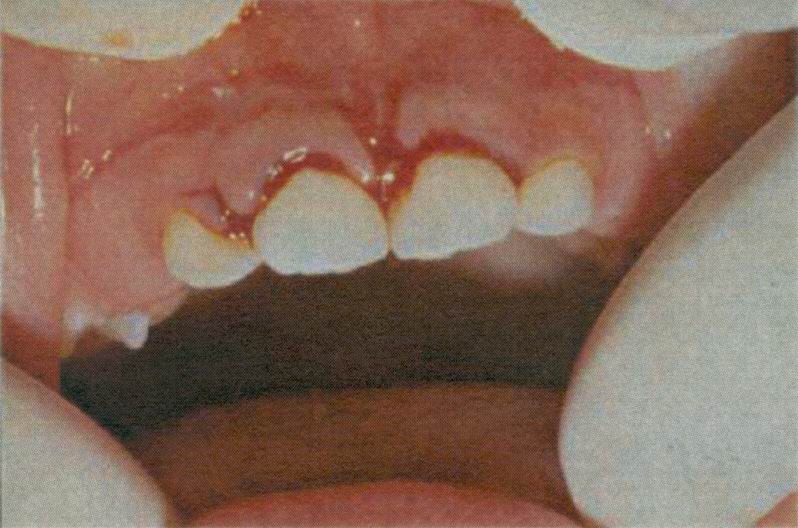
The eruption of the succedaneous teeth is often delayed after the premature loss of deciduous teeth before the beginning of their root resorption. This can be explained by the abnormal changes that might occur in the connective tissue overlying the permanent tooth and the formation of thick, fibrous gingiva. Ankylosis, resulting from the fusion of the cementum or dentin with the alveolar bone, is the most common local cause of delayed deciduous tooth exfoliation. Ankylosis occurs commonly in the deciduous dentition, usually affecting the molars, and has been reported in all 4 quadrants, although the mandible is more commonly affected than the maxilla. Ankylosed teeth will remain stationary while adjacent teeth continue to erupt through continued deposition of alveolar bone, giving the clinical impression of infraocclusion.
Ankylosis of the tooth
Arch-length deficiency is often mentioned as an etiologic factor for crowding and impactions. In a recent study of the relationship between formation and eruption of the maxillary teeth and the skeletal pattern of the maxilla, a shortened palatal length was found to delay the eruption of the maxillary second molar, although no delay in tooth formation was observed. Arch-length deficiency might lead to DTE, although more frequently the tooth erupts ectopically.
X-radiation has also been shown to impair tooth eruption. Ankylosis of bone to tooth was the most relevant finding in irradiated animals. Root formation impairment, periodontal cell damage, and insufficient mandibular growth also seem to be linked to tooth eruption disturbances due to x-radiation. Occasionally, localized DTE might be idiopathic.
Systemic conditions
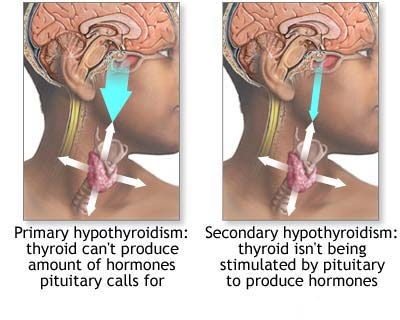 The influence of nutrition on calcification and eruption is less significant compared with other factors, because it is only at the extremes of nutritive deprivation that the effects on tooth eruption have been shown. Nevertheless, delayed eruption is often reported in patients who are deficient in some essential nutrient. The high metabolic demand on the growing tissues might influence the eruptive process. Disturbance of the endocrine glands usually has a profound effect on the entire body, including the dentition. Hypothyroidism, hypopituitarism, hypoparathyroidism, and pseudohypoparathyroidism are the most common endocrine disorders associated with DTE. In hypothyroidism, failure of thyrotropic function on the part of the pituitary gland or an atrophy or destruction of the thyroid gland per se leads to cretinism (congenital hypothyroidism) in a growing person. The dentofacial changes in cretinism are related to the degree of thyroid deficiency. In hypopituitarism or pituitary dwarfism, the eruption and shedding of the teeth are delayed, as is the growth of the body in general. The dental arch has been reported to be smaller than normal; thus it cannot accommodate all the teeth, so a malocclusion develops. The roots of the teeth are shorter than normal in dwarfism, and the supporting structures are retarded in growth.
The influence of nutrition on calcification and eruption is less significant compared with other factors, because it is only at the extremes of nutritive deprivation that the effects on tooth eruption have been shown. Nevertheless, delayed eruption is often reported in patients who are deficient in some essential nutrient. The high metabolic demand on the growing tissues might influence the eruptive process. Disturbance of the endocrine glands usually has a profound effect on the entire body, including the dentition. Hypothyroidism, hypopituitarism, hypoparathyroidism, and pseudohypoparathyroidism are the most common endocrine disorders associated with DTE. In hypothyroidism, failure of thyrotropic function on the part of the pituitary gland or an atrophy or destruction of the thyroid gland per se leads to cretinism (congenital hypothyroidism) in a growing person. The dentofacial changes in cretinism are related to the degree of thyroid deficiency. In hypopituitarism or pituitary dwarfism, the eruption and shedding of the teeth are delayed, as is the growth of the body in general. The dental arch has been reported to be smaller than normal; thus it cannot accommodate all the teeth, so a malocclusion develops. The roots of the teeth are shorter than normal in dwarfism, and the supporting structures are retarded in growth.
Retardation of dental growth and development in preterm babies has been reviewed by Seow and identified as a cause of DTE. Teething is often delayed, and Seow’s results have shown a distinct relationship between birth weight and numbers of erupted teeth. DTE is common in preterm babies with respect to the deciduous dentition, but “catch-up†development occurred in later infancy. The permanent teeth showed a significant mean delay in dental maturation of approximately 3 months in very low birth-weight babies (birth weight of _1500 g). In another study, Seow found that children with a birth weight less than 1000 g and gestational ages less than 30 weeks had the greatest lag in dental maturation.
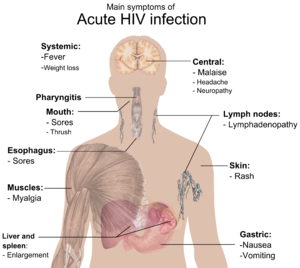 A correlation between human immunodeficiency virus (HIV) infection and DTE has also been suggested. A study of dental manifestations in 70 children perinatally infected with HIV indicates that delayed dental eruption (defined as dental age 6 or more months younger than chronologic age) was directly associated with clinical symptoms. DTE did not seem to correlate with CD4 positive T-lymphocyte depletion. The investigators concluded that HIV infection itself is not associated with DTE, but, rather, the onset of the clinical symptoms is. Another study has found that a lower tooth count at different chronologic ages in HIV-infected children might represent a marker for socioeconomic status, reflecting poorer nutrition or health. In a study of children with cerebral palsy, Pope and Curzon found that unerupted deciduous and permanent teeth were more common in them compared with the controls. The first permanent molar erupted significantly later. No etiology or implicated mechanisms were elaborated.
A correlation between human immunodeficiency virus (HIV) infection and DTE has also been suggested. A study of dental manifestations in 70 children perinatally infected with HIV indicates that delayed dental eruption (defined as dental age 6 or more months younger than chronologic age) was directly associated with clinical symptoms. DTE did not seem to correlate with CD4 positive T-lymphocyte depletion. The investigators concluded that HIV infection itself is not associated with DTE, but, rather, the onset of the clinical symptoms is. Another study has found that a lower tooth count at different chronologic ages in HIV-infected children might represent a marker for socioeconomic status, reflecting poorer nutrition or health. In a study of children with cerebral palsy, Pope and Curzon found that unerupted deciduous and permanent teeth were more common in them compared with the controls. The first permanent molar erupted significantly later. No etiology or implicated mechanisms were elaborated.