NEUROPHYSIOLOGY
The neuron is the structural unit of the nervous system. There are 2 basic types of neuron : the sensory and motor neurons
Sensory neurons that are capable of transmitting pain consist of thre major portions : the peripheral process or the dentritic zone which is composed of arborization of free neve endings, the axonal process which transmits the impulses from the dentritic process to the nuclei in the brain and the cell body or soma which provides vital metabolic support to the entire neuron.
AXON or the single nerve fibre is a long cylinder of neural cytoplasm (axoplasm) encased in a thin sheath, the nerve membrane (axolemma). The axoplasm, a gelatinous substance, is seperated from the extracellular fluids by a continous nerve membrane. The nerve cell memebrane is approximately 70 to 80 Ã… thick. The resting neve membrane has electrical resistance about 50 times greater than that of the intracellular and extracellular fluids, thus preventing the passage of ions down their concentration gradient. However, when an impulse passes, electrical conductivity of the nerve membrane inceases approximately 100-fold. This increase in conductivity permits passage of sodium ions that provides the immediate source of energy for impulse conduction along the nerve.
MODES OF ACTION
It is possible for a LA agent to interfere with the excitation process in a nerve ending in one or more way:
1)Â Â Â Â Â Â Altering the basic resting potential of the nerve membrane.
2)Â Â Â Â Â Altering the threshold potential (firing potential
3)     ↓ the rate of depolarization.
4)Â Â Â Â Â Prolonging the rate of repolarization.
MECHANISM OF ACTION
1.     Displacement of Ca++ ions from the Na+ channel receptor site  Â
2.     Binding of the LA molecule to this receptor sites
3.     Blockade of Na+ channel & a ↓ in Na+ conductance
4.     Depression of the rate of electrical depolarization
5.     Failure to achieve the threshold potential level
6.     Lack of development of propagated action potentials.
7.     conduction blockade
DISSOCIATION OF LA MOLECULES
LA’s are available as salts. In solution it exists as:
                                RNH+ ↔ RN + H+
 The RN is the base form and RNH+ is the cationic form of the drug.
The relative proportion of each ionic form varies with pH,
 At lower pH….RNH+ > RN + H+
 At higher pH…. RNH+ < RN + H+
When pKa = pH….50% RNH + & 50% RN
pKa is called the dissociation constant
The percentage of drug existing in each form can be calculated by the
Henderson- Hasselbalch equation:
                     Log  Base  = pH – pKa
                               Acid
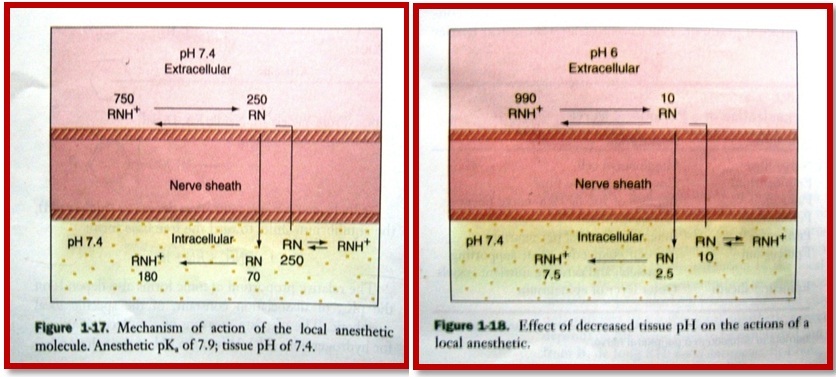
2 factors involved in the action of local anesthetic are:
Ø diffusion of the drug through the nerve sheath
Ø  binding at the receptor site
The diffusion of the drug is brought about by the base or the RN form of the drug and the RNH+Â Â or the cationic form of the drug binds to the receptor site. This can be explained with the following diagram:
PHARMACOLOGY OF LA AGENT
PHARMACOKINETICS
Absorption
When injected into the soft tissues all LA cause vasodilatation except cocaine. Procaine is a potent vasodilator
The absorption of LA depends uponÂ
1.     Route of administration
2.     Vasoconstrictor
3.     Site of injection
4.     Quantity of the drug
5.     Type and size of nerve
6.     Potency of drug
       Route of administration
·        Oral route – except cocaine all LA are poorly absorbed orally ..
·        Topical route – skin acts as a barrier to anesthetic solution …mucous membrane and injured skin permit diffusion..
·        Injection – the rate of absorption depends on the vascularity of the site and vasoactivity of the drug
Â
Distribution
Highly perfused organs like brain, liver, kidney, lungs and spleen receive higher levels of anesthetic as compared to skeletal muscles.
The blood level of LA is influenced by the following factors :
1.     Rate at which the drug is absorbed into CVS
2.     Rate of distribution from the vascular component to tissues
3.     Elimination of drug through metabolic and excretory pathways.
Â
Metabolism (Biotransformation)
Ester LA’s are hydrolyzed in plasma by the enzyme pseudo–cholinesterase. The rate of hydrolyses differs considerably. Chloroprocaine rapidly hydrolyzed and hence is least toxic. Tetracaine hydrolyzed 16 times more slowly and therefore more toxic than chlorprocaine. More allergic reactions to ester linked LA is due to Para Amino Benzoic Acid (PABA) which is a metabolite of hydrolysis of the drug. 1 out of 2800 persons has atypical pseudocholinesterase. In these patients administration of ester linked anesthetics may give rise to toxicity.
Amide LA undergoes biotransformation in Liver. Their metabolism is much more complex as compared to ester linked agents. More than 70% of these drugs metabolized in liver in normal function. In patients with low hepatic blood flow like in patients with congestive heart failure or poor liver function like hepatitis or cirrhosis, biotransformation does not occur at a normal rate and thus toxicity increases. Prilocaine produces orthotoluidine as its major metabolite which induces formation of Methhemoglobin leading to methhemoglobinemia in individuals with genetic susceptibility or patients with decreased oxygen carrying capacity. Metabolites of lidocaine (monoethylglycinexylidide and glycinexylidide) produce sedation.
Excretion
Kidneys are primary excretory organs for both ester and amide types of LA and their metabolites. A percentage of given LA is excreted unchanged. Patients with significant renal impairment are unable to eliminate the drug, leading to increased blood level and subsequent toxicity.