© pinnaclepediatricdentistry.com
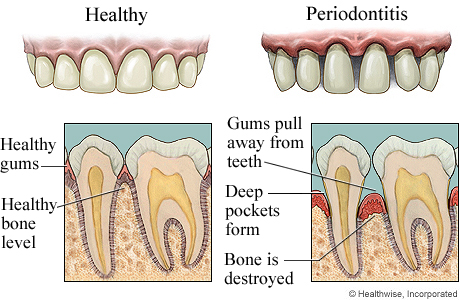
The periodontium or the commonly known as the tooth supporting tissues consists of the gums, alveolar or jaw bone, the periodontal ligament and the cementum of tooth. Numerous systemic conditions can have effects on the periodontal tissues such as:
- Physiological changes (mainly sex hormone effects)
- Systemic disease – endocrines, genetic conditions, granulomatous conditions, blood disorders, immunological conditions, dermatoses
- Infections
- Drug reactions
- Dietary and nutritional factors
This article will discuss some of the systemic factors stated above that are more commonly seen.
Physiological changes
Effects of sex hormones on the periodontium

© Intellectual Reserve, Inc.
Female sex hormones are controlled by the ovary, with analogues are used as oral contraceptives. Estrogens are involved in physiological changes in women at puberty whereas progesterones are involved in preparation of reproductive tract for fertilization. Male sex hormones are responsible for male characteristics at puberty and testosterone also promotes protein synthesis.
Estrogen promotes keratinization of epithelium and increases mucopolysaccharide content in connective tissue and progesterone increases permeability of gum blood vessels. Effects are seen during puberty, pregnancy and oral contraception. All the effects are exaggerated responses to plaque products.
Sex hormone effects on chronic periodontal disease
- Puberty – linked to more prevalence and severity of gingivitis (inflammation of the gums),
- Menstruation – linked to worsening of gingivitis at ovulation,
- Oral contraceptives – linked to worsened gingivitis over time,
- Pregnancy – special case deserving further attention. According to folklore pregnancy increases gum disease leading to tooth loss but fortunately this is not the case in well plaque-controlled mouths.
Pregnancy effects on chronic periodontal disease

Pregnancy gingivitis
Gingivitis during pregnancy starts at third month from gestation, peaks at six months with complete/partial resolution at childbirth. This is caused by an exaggerated response to plaque biofilm in the mouth due to poor oral hygiene, local irritants and a shift in the predominant types of bacteria in the mouth.
Clinical effects of pregnancy on periodontium
The gums can be bright red, swollen and sensitive with spontaneous bleeding, increase in exudates and loose teeth.
Mechanism of pregnancy gingivitis
The sex hormone progesterone increases blood supply and permeability of the blood vessels of gums with an increase of black-pigmented anaerobic bacteria beneath the gumline. Estrogen may be substituting for growth factor methadione in bacteria and serve as nutrient for bacteria to grow.
Pregnancy epulis (pyogenic granuloma of pregnancy)

Pregnancy tumor © ADCC
Pregnancy granulomas or pregnancy tumors are single, tumor-like, soft tissue growths typically seen on the gums region between teeth and they rarely destroy the bone. They are attached via a stem with intense red to deep purple color, depending on the blood supply of the lesion and the degree of blood stagnation, and bleeds easily.
This usually causes concern in expecting mothers as pregnancy epulis can sometimes painful. Pregnancy tumors usually develop after the third month of gestation with variable resolution at childbirth. This lesion often occurs due to plaque but often local secondary factors are present. Treatment is usually surgery after pregnancy and electrocautery of the lesion base.
Systemic disease – Endocrines
Effects of diabetes mellitus on the periodontium
Diabetes mellitus is a metabolic disorder characterized by glucose intolerance. There are two main types of diabetes mellitus:
- Type 1 or Insulin Dependent diabetes – with 2% incidence, sudden onset of diabetes begins prior to 25 years of age. Type 1 diabetes is characterized by the sudden appearance of thirst, frequent urination, hunger, and weight loss. This disorder of Islets of Langerhans requires daily insulin injections for control.
- Type 2 or Non-insulin Dependent diabetes –mainly affecting obese middle-aged people, Type 2 diabetes is characterized by slow onset and includes any other type of the type 1 symptoms. This disorder is controlled by diet and hypoglycemic drugs.
Complications of diabetes mellitus include atherosclerotic changes in the arterioles, capillaries and venules; wide range of organs with significant kidney, eye and nerve changes, and increased glucose in tissues which may promote infectious processes.
Diabetes mellitus and periodontal disease
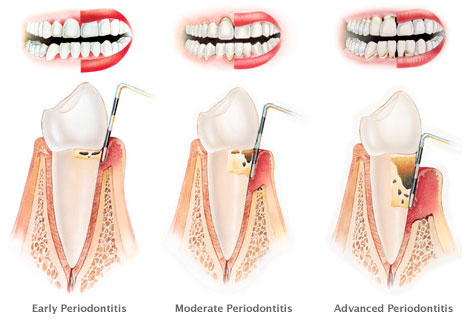
Levels of chronic periodontitis © Stanley Dentistry
The prevalence and severity of periodontal diseases are increased in individuals with both type 1 and type 2 forms of diabetes especially severe uncontrolled type 1 diabetes. Â Well-controlled diabetic are not at greater risk of periodontitis though, longstanding diabetics with complications have more risk of periodontal disease
A two-way relationship exists between periodontal disease and diabetes. Periodontal disease appears to complicate diabetes by making control of blood glucose levels more difficult. Diabetic individuals who have weak immune systems are more likely to acquire bacterial infection associated with periodontal disease.
Alterations produced by diabetes that affect the periodontium
- Effects of vascular changes and impaired polymorphonuclear leucocytes (PMN) chemotaxis that decreases immune response,
- Increased collagen cross-linking making it less susceptible for breakdown leads to increase in accumulation of advanced glycation end products (AGE) which increases amount of old collagen resulting in weakness of the periodontium,
- Increased amount of anaerobic flora due to increased glucose levels leads to a shift in bacteria flora.
Preventative strategies in diabetes patients
Nearly all diabetics respond to treatment and maintenance therefore prompt treatment of any periodontal infections should be done with antibiotic cover if periodontal surgery is required.
To be continued in Part 2