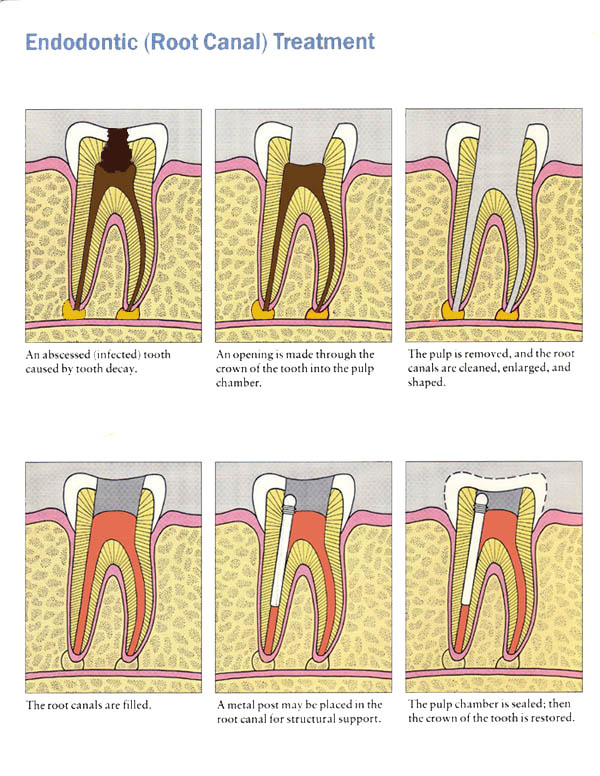
INTRODUCTION:
Clinical endodontics has changed and expanded over the years due to improvement in cleaning and shaping procedure,culturing, intra canal medicaments and root canal filling materials and techniques
Definition:
It is defined as the conservative non surgical treatment of an endodontically involved tooth consisting of complete biomechanical cleaning , shaping and obturation of the root canal system during one visit.
Preliminary considerations:
a) Operator ability and clinical experience: It requires highest level of competence of practitioner who have made endodontics as an integral part of
clinical practice.
b) Time and auxiliary utilization (30-45min)
c) Dependent on efficient endodontic delivery system .
d) Requires well trained dental assistant .
Clinical techniques
Indications
1. Isolation and sealing problems
2. In cases of teeth with subgingival break down, multiple coronal walls missing and teeth with full coverage that have decay below the margins.
3. Anterior esthetic problems
4. Restorative considerations
a) Teeth to be used as over denture abutments
b) Mandibular anteriors
c) Teeth with severe coronal breakdown
Vital pulp exposures and symptomatic pulpitis.
5. Asymptomatic nonvital pulp
Contraindications
1) Periapical symptoms with or without swelling
2) Anatomic problems
Calcified canals
Sharply curved canals
Bifurcated canals
Dilacerated canals
Receded pulp chambers
3) Multirooted teeth
4) Retreatment cases
Advantages
It reduces patient appointment visits.
It eliminates inter appointment contamination or flare ups
It allows the practitioner to immediately use the canal for retention of a post to construct an esthetic temporary.
Disadvantages
In case of retreatment or flare ups ,may have to do artificial fistulation or trephination
Time consuming in molars
Post Endodontic Restorations
GENERAL CONSIDERATIONS FOR RESTORATION
Brittleness of tooth structure
Loss of tooth structure
Discoloration of tooth structure
Margin 1-5mm below gingival sulcus
Objective of restoration of endodontically treated tooth consists of 3 R’s
1. Reinforcement of remaining tooth structure is achieved
by dowel and coping.
2. Replacement of missing tooth is achieved by the core.
3. Retention is supplied by the post or dowel for the core
and the core supplies retention for the final restoration.
Basic components of the post endodontic restoration are 4 :
Posts
Pins
Cores
Final restoration
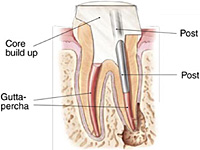
In post and core fabrication, it is desirable that the post descend at least two third of the length of root canal (or not less than the height of the crown) in order to provide sufficient retention.
Basically, it is important to leave at least 5 mm of gutta percha at the apex of the root canal, even at the expense of a longer post, because it is within the apical 5 mm of the root canal that the apical delta anastomose with the exterior surface of the root. Should these lateral canals not be blocked with the gutta percha and the cement used to place the gutta percha, the chances of microleakage and percolation of microbes are greatly increased, thereby increasing the likelihood of an endodontic failure.
It is not necessarily the length of the post within the root canal that provides for retention of the core, and thus the eventual crown, but rather the length of post that will exist within root structure that exists within surrounding bone. If the post is 16 mm long, but only extends 4 mm into root structure that is surrounded by solid bone, the restoration will have a poor prognosis. This consideration of crown-to-root ratio is essential when evaluating the tooth for a crown lengthening procedure.
In the picture at right, the two teeth on the extreme left and right are the ones under discussion. The two teeth in the middle have been endodontically treated, but do not have post and cores.
POSTS:
Why and when it is used
Selection of root for post
Posts:
Cemented or threaded into prepared channel to retain the restoration and protect remaining tooth structure
Types:
Custom made
Pre fabricated
According to Walton: a) Actively placed post
b) Passively placed post
Prefabricated:
Tapered smooth
Parallel cemented
Parallel with tapered apical end
Tapered self threading
Parallel threaded.
Custom made:
Where post and core are one unit, this can be made by direct or indirect method.
III: Esthetic ex: Glass fibre posts and ceramic posts
non-esthetic ex: metallic posts.
Posts contraindicated in:
Severely curved canal
Canals filled with materials that are non-resorbable like resins materials and silver cones.
Whenever coronal structure is sound and adequate
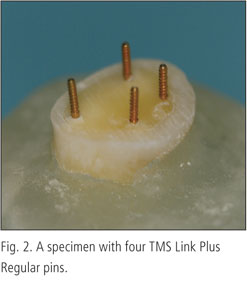
PINS:
Used alone and in combination, to provide retention for core material
In some cases posts cannot be used to provide retention
CORE:
Replaces coronal tooth structure that has been lost due to caries and previous restoration. It provides a base that has sufficient bulk and retention for final restoration. Amalgam / Composite or may be cast restoration in precision or non-precision alloy in combination with posts.
POST SPACE PREPARATION:
i.e. Removal of G.P by hot pluggers or spreaders simultaneously shaping with peeso reamer or GGD.
Direct method of post and core
Indirect method of post and core
Cementing media for posts is ZnPO4 or Zn polycar
When prefabricated posts are used core is made either with composite or amalgam.
FINAL RESTORATION:
Usually full veneer crown – posteriors
Anteriors – porcelain crowns. Needs shoulder finish line
For cast metal – chamfer type of finish line
Shoulder and chamfer should be used in natural tooth structure
To obtain
Adequate retention
To protect remaining tooth structure
To restore occlusal function
To provide properly contoured axial surface
Use esthetic veneers in cosmetic considerations