The purpose of root canal treatment with baby teeth is to keep the teeth in function until exfoliation, or at least for as long as they are important for occlusal development. Besides eating and speaking, many parents do not know that baby teeth (or primary teeth) also act as a guide for the underlying permanent teeth to erupt and at the same time they maintain the space on the arch so that the permanent teeth has enough room to grow when it is out.
Â
Root Canal or Extraction?
Important factors to consider are the baby teeth’s diagnosis, overall teeth conditions and child’s general and oral health. However, the choice between root canal and extraction will be based on the value of the tooth for future occlusal development and the child’s ability to cooperate with the treatment. For example, if there is any risk of injury or infection of the underlying permanent tooth, extraction should be preferred. Consequently, root canal is relevant for cases with infected or decayed primary teeth before the time of eruption of the permanents.
Â
Root Canal Techniques in Primary Teeth
All root canal treatment will be performed under asepsis condition, means that the tooth will be isolated with a rubber dam and the tooth and the operation area are disinfected before the treatment.

Rubber dam use to isolate the tooth to avoid contamination (bacterial, saliva) from oral cavity.
Â
Â
1. Stepwise Excavation or Indirect Pulp Capping
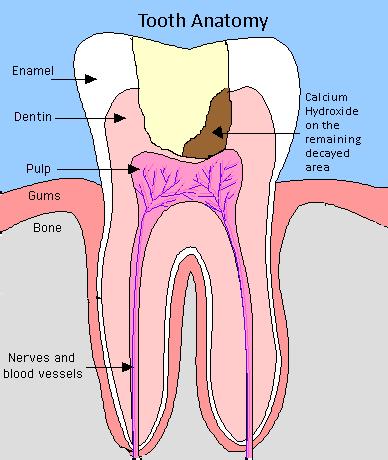
Indirect pulp capping
Â
Indications: Deep carious lesion, carious softened tissue close to pulp but no exposure. No clinical or slight radiographic signs of pulpitis. Pulpitis is an inflammation of the pulp tissue of a tooth.
Â
The technique includes removal of most of the soft decayed dentin but do not expose the pulp. Remaining decayed portion is covered with Calcium Hydroxide and left temporarily under an intermediate filling. The tooth is left for at least 3 to 6 months while a hard tissue barrier is formed. This means that less or no risk of exposing the pulp when re-entering the area to removal the remaining carious lesion and a permanent tooth filling is given thereafter.
Â
2. Partial Pulpotomy
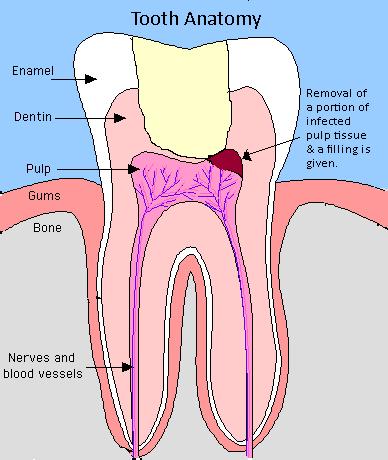
Partial pulpotomy
Â
Indications: Accidental exposure of healthy pulp, carious exposure – partial chronic pulpitis or symptomless carious exposure.
Â
Partial pulpotomy is the surgical removal of a portion of the pulp tissue. This technique includes removal of a small part of the pulp just at the site of exposure, application of Calcium Hydroxide in direct contact to the wound surface and a permanent filling is given. This technique is advantageous because there is good access to the pulp wound, sufficient space for the wound dressing and establishment of a tight seal against the oral environment (for example, saliva)Â with the permanent filling right after the procedure.
Â
3. Pulpotomy
Pulpotomy: Wound dressing placed in the orifices of the root canals.
Indications: Large carious exposure (badly decayed tooth)– pulpitis, partial or total chronic pulpitis (symptomless carious exposure), absence of abscess or swelling, instances where extraction is contraindicated e.g. hemophilia children.
Â
Pulpotomy is the surgical removal of the pulp tissue only on the crown of the tooth. This techniques and the treatment of the wound are the same as described for partial pulpotomy, but the wound area is much deeper.
Â
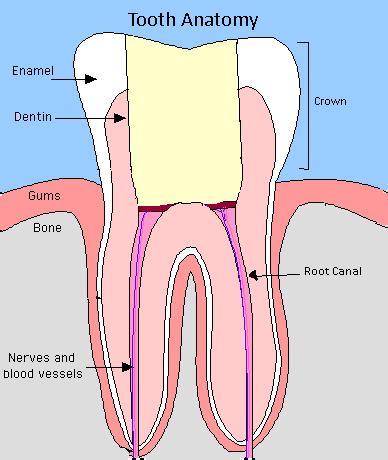
4. Pulpectomy
Pulpectomy
Â
Indications: Irreversible pulpitis involving the entire pulp tissue, non-vital primary teeth that needed to be maintained in the arch, abscessed primary molars, primary molars with radiographic evidence of pathology.
Â
Pulpectomy is the surgical removal of the entire pulp tissue from the root canal. This technique includes disinfection and cleaning of the root canals, root length is determined, filling of root canal with resorbable wound dressing (Calcium Hydroxide or Zinc Oxide Eugenol) followed by placement of a filling. The reason of using a resorbable dressing is to avoid affecting the permanent teeth to erupt. The modern approach is to avoid pulpectomy in baby teeth and to choose extraction. As mentioned before, the risk of injury the underlying permanent teeth should be taken into account.
Â
Conclusion
Despite all the techniques above, it is reasonable to consider the necessity and outcome of the treatment planned. Hence, it is not ethically justifiable to let a child undergo treatment if the outcome is uncertain or poor because performing a root canal treatment on a child does include some discomfort and strain. All in all, the prognosis of this treatment is fairly favorable.