
© Imagine Orthodontics
If you have a space between your upper front teeth like the photo shown above, it means that you are having midline diastema. In dental terms, midline diastema refers to an anterior midline spacing between the two maxillary central incisors. It is one of the most frequently seen malocclusions that is considered easy to treat but often difficult to retain.Â
Causes and treatment of midline diastema :
1 ) Temporary malocclusion / Normal Developing Dentition : This condition is seen during ugly duckling stage of children aged between  8-9 years old after the eruption of central incisors.
Treatment : Â This condition usually corrects by itself when the canines erupt and the pressure is transferred from the roots to the coronal area of the incisors.

2) Abnormal frenal attachment : The presence of a thick and fleshy frenal labial attachment can give rise to a midline diastema. This kind of frenal attachment prevents the two central incisors from approximating each other due to the fibrous connective tissue interposed between them.
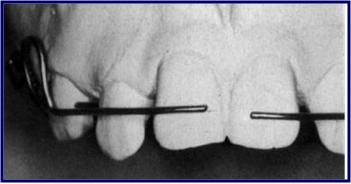
BLANCH TEST:- Lift the upper lip and pull in outward and look for blanching of the soft tissues lingual to and between two central incisors.
Presence of blanch indicates high frenal attachment as cause of midline diastema.
Treatment : Frenectomy should be performed. Generally advocated that the diastema should be closed as far as possible before going in for frenectomy. The reason cited is that should the surgery be performed before the surgical scar tissue maintains the diastema.
3) TOOTH MATERIAL DEFICIENCY

Microdontia
a) Microdontia
Microdontia refers to teeth that appear smaller in size compared to normal.
In this case the jaw size is normal but the size of the teeth is small which produces diastema between the teeth.
Microdontia is most frequently seen in Down’s syndrome and ectodermal dysplasia.
b) Macrognathia
It is a developmental anomaly characterized by an abnormal large jaw.In this case the size of the tooth is normal but because of the increase in size of jaw, it results in diastema.
Missing Lateral Incisors
c) Missing lateral
Due to the missing lateral there will be tooth material-arch discrepancy as a result there will be drifting of adjacent teeth.
d) Extracted tooth
This also results in tooth material-arch discrepancy which causes drifting of adjacent teeth.
Treatment : Â

Jacket Crown
DIASTEMA DUE TO MICRODONTIA AND MACROGNATHIA
Such conditions can be treated by orthodontic means or by mean of jacket crowns or composite build-up.
Closure by jacket crown or composite build-up is the best method.
DIASTEMA DUE TO MISSING TEETH/EXTRACTED TOOTH
Space can be consolidated and replaced with implant or bridge
4)Â RACIAL PREDISPOSITION
The presence of midline spacing also has a racial and familial background.
The negroid race shows the greatest incidence of midline diastema.
5) Â HABITS
a) Thumb sucking
Thumb sucking is defined as placement of the thumb or one or more fingers in various depths into the mouth.
It can cause severe proclination of the maxillary anterior teeth along with formation of diastema
b) Tongue thrusting
This is a condition in which the tongue makes contact with any teeth anterior to the molars during swallowing.
It also causes proclination of anterior teeth along with diastema and open bite.
Treatment : Habit Breaking Appliances
c) Frenum thrusting
This habit is a self injurious habit.
If the maxillary incisors are slightly spaced apart, the child may lock his labial frenum between these teeth and permit it to remain in this position for several hours.
6) PHYSICAL IMPEDIMENT
a) Retained deciduous teeth.
This causes ectopic eruption of tooth and formation of median diastema.
b) Mesiodens
Presence of an unerupted mesiodens between the two central incisors also predispose to midline diastema.
c) Abnormal labial frenum
The presence of a thick and fleshy labial frenum can cause a midline diastema.This type of fibrous attachment can prevent the two maxillary central incisors from approximating each other.
d) Midline pathology
Soft tissues and hard tissue pathologies such as cysts, tumors and odontomes may cause midline.
ACTIVE TREATMENT
A) REMOVABLE APPLIANCES
Split Labial Bow
Simple removable appliances incorporating finger springs or a split labial bow can be used.
Finger springs can be given distal to the two central incisors.
Split labial bow made of a 0.7mm hard stainless steel wire can be used.
In a reciprocal tooth movement the forces are applied to teeth Fare equal and opposite as a result each unit moves to a normal occlusion.

A) Closure of a midline diastema can be accomplished with a removable appliance and finger springs to tip the teeth mesially. B ) The 28 mil helical finger springs are activated to move the incisors together. C ) The final position can be maintained with the same appliance.
FIXED APPLIANCES

Fixed appliances incorporating elastics and springs bring about the most rapid correction of midline diastema.
Elastics can be stretched between the two central incisors in order to close the space.
Elastic thread or elastic chain can be used between the central incisors.
M shaped springs incorporating three helices can be inserted into the two central incisor brackets.
The spring can be activated by closing the helices.
Closure of a diastema with a fixed appliance A.) This diastema requires closure by moving the crowns and roots of the central incisors. B ) The bonded attachments and rectangular wire control the teeth in three planes of space while the elastomeric
chain provides the force to slide the teeth along the wire. C) immediately after space closure, the teeth are retained, preferably with, (D) a fixed lingual retainer at least until the permanent canines erupt.
 RETENTION
Midline diastema is often considered easy to treat but difficult to retain.
Retention can be achieved by:-
Lingual bonded retainers
Banded retainers
Hawley’s retainer
NEWER APPROACH
ROLE OF COSMETIC RESTORATION
Esthetic composite resins are used to close midline diastema especially in adult patients.
It requires gradual composite build up on the mesial surface and stripping of the distal surface of centrals and laterals in order to achieve a natural shape and size of the teeth.
PROSTHESIS/CROWN
Presence of peg shaped laterals or teeth with other anomalies of shape and size require prosthetic rehabilitation.
Missing teeth should be replaced with fixed or removable prosthesis