We hear from a lot of denture wearers that tell us stories about having a lot of difficulty eating the foods that they want and need to eat, in speaking clearly, and with their appearance. To solve these problems, we use a more involved denture technique called the Branching Technique. The “branching technique,” taught first by Pound and later by Turbyfill and others, allows for extended treatment and management of more complex patient problems.  Less than 1% of dentists in the United States use this technique because of the great amount of training required to learn it, as well as more time spent on working with the patient.Â

Inflamed gum tissue preventing proper impression taking for fabricating denture
The Branching Technique differs from the traditional method whereby experimental dentures are constructed and approved by patient and dentist before the final dentures are constructed. It is a protective philosophy for both patient and dentist. It is a “try it before you buy it†philosophy. Unlike the conventional “linear†methods which follow specific steps in a cookbook fashion, the Branching Technique is a dynamic concept which can be adjusted to meet the clinical needs of each patient.  A “training denture†is used to treat the inflamed gum tissue, establish the bite, develop the aesthetics, and make an impression that perfectly fits the gums before the final denture is made. The “training denture†is a temporary denture that contains a soft, conforming material inside that is worn for several weeks while chewing food, smiling, talking etc. The impression is much more accurate, and makes an ideal and more practical impression of the gums and surrounding tissues. It basically provides a perfect blueprint for the final denture. Fit the patient with the permanent denture once it is completed, and check for any issues with bite alignment and comfort level. This is not a quickie mass production technique, but designed for dentists who want the ultimate in full denture service for their patients. However, there is a way that our basic technique can be incorporated into a short denture procedure.
Follow up with the patient a week or so after the denture is completed and taken home. Invite the patient to come in for an examination if he/she is experiencing any discomfort, alignment difficulties or general struggles with usage. Recommend a denture cleaner, and other wear and care tips that the patient can carry with him/her through the week.

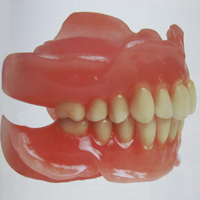
The cosmetics on the dentures are amazing
This method has given tremendous success for the patients as a great deal of time was spent on designing the teeth for their overall look. Dentures have to look and feel natural, they’ve got to fit the gums properly, and the bite must be flawless. Only the finest denture teeth are used, carefully selected to compliment the size, shape, and color of the person’s mouth and face. Teeth are set in an individualized manner, considering each person’s gender, age, and personality. A built-in “soft-cushion†liner is also used for some lower dentures to insure maximum comfort. The “gum†portions can also be shaded and textured to make them appear exceptionally real. The cosmetics on the dentures are amazing and patients who have used them tells that their friends think they’ve had a smile makeover, instead of thinking they now wear dentures.
The development of osseointegrated root form implant systems has taught us one thing about patients who are dental cripples – they are willing to invest large amounts if the profession has something better to offer. Most denture patients know as well as the dentist the old impression, jaw relation, try-in and delivery system and they know all too often multi post-operative adjustments that lead to dissatisfaction. The Branching Technique is generally readily accepted by the patients.
Branching Technique Objectives for Dentists and Dental Technologist:
-

Balanced occlusion in centric relation
Arrange maxillary and mandibular teeth to esthetics using anatomical harmony and phonetics with no chance of restriction of the anterior envelope of function
- Achieving a balanced occlusion in centric relation using several procedures. Occlusion is the single most important principle in removable prosthetics.
- Delivery of the treatment denture and achievement of perfect patient generated functional impressions.
- Lingualized occlusion as well as when to use cross bite
- Treating Class I, II and III cases using the same basic principles.
- Finalization procedures to go from the treatment denture to the final denture that require few if no post insertion adjustments.
- Occlusal refinement using a central bearing point and functional analysis of the envelope of function.
- Use of the treatment denture to make a surgical stint and for the prosthetic guide if implants are part of the treatment options.
- Custom gold occlusal surfaces in removable appliances.
- Sometimes the use of plastic teeth can cause problems for the patient in the future.
- Basic partial denture design principles. Keeping attachments simple. Post insertion reline of the free end saddle partial to assure success.