Suckling vs. sucking
Suckling
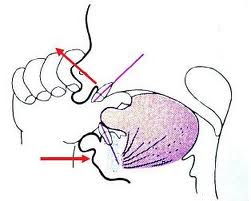
Suckling is a normal physiological reflex in infants, which consists of small nibbling movements of the lips. The movements stimulate the smooth muscles surrounding the milk ducts of the lactating mother to contract and squirt milk into the infant’s mouth. When the milk is squirted into the mouth, it is only necessary for the infant to groove the tongue to allow the milk to flow back into the throat. The tongue, however, must be placed front to contact with the lower lip, so that the milk is in fact deposited on the tongue. The tongue-to-lip apposition is so common that it is usually adopted at rest, and it is frequently possible to gently move the infant’s lower lip and notice that the tongue tip moves with it, almost as if they were glued together. The suckling reflex normally disappears during the first year of life.
 Sucking
Sucking
Nearly all modern infants engage in some sort of habitual non-nutritive sucking– thumb- or finger-sucking or sucking of a similarly shaped object. A vast majority do so during the period from 6 months to 2 years or later.
How can thumb sucking affect the development of teeth?
As a general rule, sucking habits during the baby teeth (primary dentition) years have little if any long-term effect. However, if these habits persist beyond the time that the permanent teeth begin to erupt (mixed dentition years), malocclusion characterized by flared and spaced upper front teeth, a vertical space between upper and lower front teeth (anterior open bite), and a narrow upper dental arch is a likely result. The characteristic malocclusion associated with sucking arises from a combination of direct pressure on the teeth and a change in the pattern of resting cheek and lip pressures. The degree of malocclusion depends on the intensity, duration, and frequency of the habit.
Types of malocclusion caused by thumb sucking
- Displacement of front teeth
When a child places a thumb between the upper and lower front teeth at an angle so that it directly presses against the lower front teeth towards the tongue and against the upper front teeth towards the upper lip, there can be considerable variations in the teeth which are affected, depending on which teeth are contacted. How much the teeth will be displaced should correlate better with the number of hours per day of sucking than with the magnitude of pressure. -

Anterior open bite It arises by a combination of interference with normal eruption of front teeth and excessive eruption of back teeth. When the thumb is placed between the front teeth, the lower jaw must be positioned downward to accommodate it. Hence, the interposed thumb directly impedes the eruption of front teeth and the separation of jaws alters the vertical equilibrium on the back teeth, leading to more eruption of the back teeth. 1mm of elongation of the back teeth opens the bite by approximately 2mm in the front teeth.Narrowed/ constricted upper dental arch The dental arch form is affected by an alteration in the balance between cheek and tongue pressures. Lowered tongue position (to accommodate the thumb) decreases the tongue pressure against the upper back teeth and at the same time increases the cheek pressure against these teeth as the cheeks contract during sucking. Cheek pressures are the greatest at the corner of the mouth. This probably explains why the upper arch tends to become V-shaped, with more constriction across the canine teeth than the molar teeth.What can be done if my child develops the malocclusion?Sucking does not create a severe malocclusion unless the habit persists until the permanent teeth start to erupt (into mixed dentition years). If the child stops sucking before this stage, normal lip and cheek pressures soon restore the teeth to their usual positions.
If the habit persists after the permanent teeth begin to erupt, orthodontic treatment may be necessary to overcome the resulting crooked teeth. The constricted upper dental arch is the aspect of malocclusion least likely to correct spontaneously. If the upper arch is expanded sideways (by orthodontic therapy), both the flared upper front teeth and anterior open bite will improve spontaneously.
If the sucking habit stays even after the therapy, the malocclusion tends to relapse. So there is no point starting orthodontic treatment until the habit has stopped.